2022年 第8卷 第1期
《工程(英文)》 >> 2022年 第8卷 第1期 doi: 10.1016/j.eng.2020.05.014
预测新型冠状病毒肺炎患者临床预后好转概率的列线图—— 以中国浙江省为例
a State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, National Clinical Research Center for Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou 310003, China
b State Key Laboratory of Genetic Engineering, Institute of Biostatistics, School of Life Sciences, Fudan University, Shanghai 200433, China
c Division of Hepatobiliary and Pancreatic Surgery, Department of Surgery, Key Lab of Combined Multi-organ Transplantation of the Ministry of Health, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou 310003, China
d Division of of Endocrinology and Metabolism, Department of Internal Medicine System, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou 310003, China
# These authors contributed equally to this work.
下一篇 上一篇
摘要
本研究旨在为临床医生开发一种定量方法,以预测新型冠状病毒肺炎(COVID-19)患者临床预后好转的可能性。本研究收集了2020年1月10日至2月26日入院后经实验室确诊的104例COVID-19感染患者的数据,包括患者的临床基本信息和实验室检查结果,并比较好转和未好转患者的各项参数。本研究使用最小绝对收缩和选择算法(LASSO)logistics 回归模型和双向逐步策略的多因素logistics 回归模型筛选预测预后因素,使用一致性指数(C指数)评估模型,并通过重复抽样进行内部验证,以此构建了一项新的预测列线图。截至2020年2月26日,研究中包括的104位患者(中位年龄为55岁)中,75位(72.1%)预后好转,而29位(27.9%)没有明显好转迹象。临床预后好转的患者与未好转的患者在临床特征和实验室检查结果上存在许多差异。经过多步筛选过程后,本研究筛选出5项预后因素并将其纳入列线图的构建,包括免疫球蛋白A(IgA)、C反应蛋白(CRP)、肌酸激酶(CK)、急性生理学和慢性健康评估表II(APACHE II),以及CK和APACHE II之间的相互作用。本研究建立的模型的C指数为0.962 [95%置信区间(CI)为0.931~0.993],并且通过重复抽样验证其值仍然达到0.948。预测列线图与理想模型相比,在校准图方面显示出接近的性能,并且决策曲线和临床影响曲线显示,其在临床上具有实用性。本研究构建的列线图有助于临床医生预测每位COVID-19患者的临床预后好转的可能性,将有助于个性化的咨询和治疗。
关键词
图片

图1
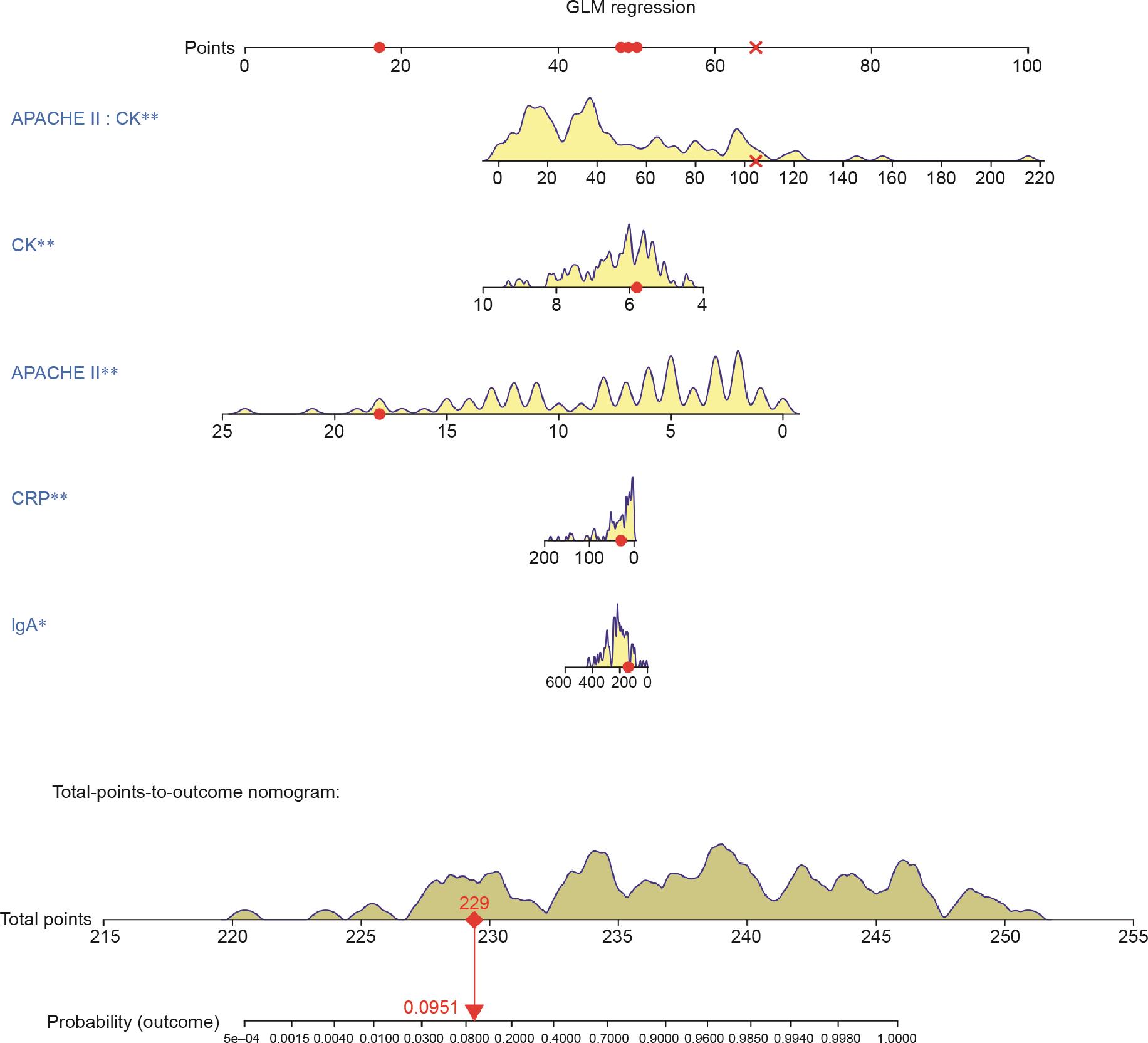
图2

图3

图4

图5
参考文献
[ 1 ] Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020;395 (10223):497–506. 链接1
[ 2 ] Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 2020;395(10223):507–13. 链接1
[ 3 ] World Health Organization. Naming the coronavirus disease (COVID-19) and the virus that causes it [Internet]. Geneva: Word Health Organization; c2020 [cited 2020 Feb 11]. Available from: https://www.who.int/emergencies/ diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirusdisease-(covid-2019)-and-the-virus-that-causes-it. 链接1
[ 4 ] Holshue ML, DeBolt C, Lindquist S, Lofy KH,Wiesman J, Bruce H, et al. First case of 2019 novel coronavirus in the United States. N Engl J Med 2020;382(10):929–36. 链接1
[ 5 ] Xu X, Wu X, Jiang X, Xu K, Ying L, Ma C, et al. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: retrospective case series. BMJ 2020;368:m606. 链接1
[ 6 ] Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med 2012;367:1814–20. 链接1
[ 7 ] Zhong N, Zheng B, Li Y, Poon, Xie Z, Chan K, et al. Epidemiology and cause of severe acute respiratory syndrome (SARS) in Guangdong, People’s Republic of China, in February, 2003. Lancet 2003;362(9393):1353–8. 链接1
[ 8 ] Guan W, Ni Z, Hu Y, Liang W, Qu C, He J, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 2019;2020(382):1708–20. 链接1
[ 9 ] nhc.gov.cn/[Internet]. Beijing: National Health Commission of the People’s Republic of China; [cited 2020 Mar 3]. Available from: http://www.nhc.gov.cn. Chinese. 链接1
[10] Coronavirus Disease (COVID-19) Dashboard [Internet]. Geneva: Word Health Orgainization; c2020 [cited 2020 Mar 2]. Available from: https://covid19.who.int. 链接1
[11] Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 2020;323(11):1061–9. 链接1
[12] Peng J, Wang M, Ang IYH, Tan SHX, Lewis RF, Chen J, et al. Potential rapid diagnostics, vaccine and therapeutics for 2019 novel coronavirus (2019- nCoV): a systematic review. J Clin Med 2020;9(3):623. 链接1
[13] Clinical management of severe acute respiratory infection when COVID-19 is suspected: interim guidance [Internet]. Geneva: World Health Organization; c2020 [cited 2020 Mar 13]. Available from: https://www.who.int/publicationsdetail/clinical-management-of-severe-acute-respiratory-infection-when-novelcoronavirus-(ncov)-infection-is-suspected. 链接1
[14] Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med 1985;13(10):818–29. 链接1
[15] National Health Commission of the People’s Republic of China; National Administration of Traditional Chinese Medicine. Guidelines for diagnosis and treatment of novel coronavirus pneumonia (trial version 7) [Internet]. Beijing: The State Council of the People’s Republic of China; 2020 Mar 3 [cited 2020 Mar 4]. Available from: http://www.gov.cn/zhengce/zhengceku/2020-03/04/ 5486705/files/ae61004f930d47598711a0d4cbf874a9.pdf. Chinese. 链接1
[16] Al Ghamdi M, Alghamdi KM, Ghandoora Y, Alzahrani A, Salah F, Alsulami A, et al. Treatment outcomes for patients with Middle Eastern respiratory syndrome coronavirus (MERS CoV) infection at a coronavirus referral center in the Kingdom of Saudi Arabia. BMC Infect Dis 2016;16:174. 链接1
[17] Wu J, Xu F, Zhou W, Feikin DR, Lin C, He X, et al. Risk factors for SARS among persons without known contact with SARS patients, Beijing, China. Emerg Infect Dis 2004;10(2):210–6. 链接1
[18] Saad M, Omrani AS, Baig K, Bahloul A, Elzein F, Matin MA, et al. Clinical aspects and outcomes of 70 patients with Middle East respiratory syndrome coronavirus infection: a single-center experience in Saudi Arabia. Int J Infect Dis 2014;29:301–6. 链接1
[19] Feikin DR, Alraddadi B, Qutub M, Shabouni O, Curns A, Oboho IK, et al. Association of higher MERS-CoV virus load with severe disease and death, Saudi Arabia, 2014. Emerg Infect Dis 2015;21:2029–35. 链接1
[20] Majumder MS, Kluberg SA, Mekaru SR, Brownstein JS. Mortality risk factors for Middle East respiratory syndrome outbreak, South Korea, 2015. Emerg Infect Dis 2015;21(11):2088–90. 链接1
[21] Ahmed AE. The predictors of 3- and 30-day mortality in 660 MERS-CoV patients. BMC Infect Dis 2017;17:615. 链接1
[22] Nam HS, Park JW, Ki M, Yeon MY, Kim J, Kim SW. High fatality rates and associated factors in two hospital outbreaks of MERS in Daejeon, the Republic of Korea. Int J Infect Dis 2017;58:37–42. 链接1
[23] Leung TW, Wong KS, Hui AC, To KF, Lai ST, Ng WF, et al. Myopathic changes associated with severe acute respiratory syndrome: a postmortem case series. Arch Neurol 2005;62(7):1113–7. 链接1
[24] Ko JH, Park GE, Lee JY, Lee JY, Cho SY, Ha YE, et al. Predictive factors for pneumonia development and progression to respiratory failure in MERS-CoV infected patients. J Infect 2016;73(5):468–75. 链接1
[25] Liew FY, Russell SM, Appleyard G, Brand CM, Beale J. Cross-protection in mice infected with influenza A virus by the respiratory route is correlated with local IgA antibody rather than serum antibody or cytotoxic T cell reactivity. Eur J Immunol 1984;14(4):350–6. 链接1
[26] Otten MA, van Egmond M. The Fc receptor for IgA (FcalphaRI, CD89). Immunol Lett 2004;92(1–2):23–31. 链接1











 京公网安备 11010502051620号
京公网安备 11010502051620号




