
《1. Introduction》
1. Introduction
Rheumatoid arthritis (RA) is a complex disease that is difficult to treat; it affects people worldwide and exhibits limited complete remission following treatment with current existing medicines, while creating a considerable burden on families and society [1–3]. The global prevalence of RA is approximately 0.5%–1% [4,5], with a 2–3 times higher rate in females than males [6,7]. The pathogenesis of RA has not yet been well defined due to its complicated mechanism, which involves systemic autoimmune manifestations in multiple tissues, organs, and systems [1,2,8,9]. In addition, the high recurrence rate of RA leads to long-term or even lifetime treatment for patients. The key strategy for treating RA is early diagnosis and early treatment to prevent further disease progression; however, the available methods remain unsatisfactory [10].
Disease-modifying anti-rheumatic drugs (DMARDs) are the first-line therapy for RA, and have been shown to inhibit disease progression and bone erosion [11]. However, DMARDs may induce severe side effects that lead to the discontinuation of treatment by nearly one-third of patients due to drug intolerance [12,13]. Among the 20 million patients with RA who have been treated with DMARDs, 7 million failed to achieve clinical remission or produced only partial responses [14]. In the past two decades, the invention of biological agents has advanced RA treatment [11,15]; unfortunately, less than 10% of patients with RA in China are able to afford biological therapies [16,17], and not all patients who can afford biological agents experience relief after fullcourse therapy [18]. Moreover, an increased risk of infectious outcomes, including opportunistic infections, has been observed among users of tumor necrosis factor (TNF) antagonists (40.1%) compared with people treated with methotrexate (MTX; 30.9%) [19]. In addition, patients with RA who are selected for TNF inhibitor treatment show a 50% increased risk of invasive melanoma [20]. These results may restrict the wide application of biological agents, particularly in patients with RA who are diagnosed with hepatitis B, hepatitis C, tuberculosis (TB), malignant tumors, severe infections, or pregnancy. Thus, an imperative mission for rheumatologists and basic researchers is to identify safer and more costeffective medications; traditional Chinese medicine (TCM) may provide some new options.
TCM treatments have become increasingly popular in China and other Asian countries for refractory diseases, while the reputation of TCM has been enhanced worldwide. Approximately 75% of Chinese or immigrant Chinese patients prefer TCM or other complementary and alternative medicines for arthritis, musculoskeletal conditions, fatigue, and health maintenance [21], but this proportion remains much lower in the western world. Several studies have been performed in China over the past few decades to accelerate the transformation of TCM from an experiencebased medicine to an evidence-based medicine; these reports have greatly enhanced the acceptance of TCM treatments and the scientific reputation of TCM worldwide. For example, Prof. Youyou Tu was awarded the Nobel Prize in Physiology or Medicine in 2015 for her discovery of artemisinin as a malaria treatment [22,23], while Dr. Zhu Chen won the 2018 Sjoberg Prize and the 2016 Ernest Beutler Lecture and Prize for developing a novel targeted treatment strategy using all-trans retinoic acid (ATRA) and TCM–arsenic trioxide (As2O3) combination therapy, which transformed acute promyelocytic leukemia (APL) from a highly fatal disease into the first curable acute myeloid leukemia [24,25]. These high honors are the most outstanding examples of researchers who have explored and applied TCM to cure severe human diseases through integral research of TCM and cutting-edge multidisciplinary technologies. These and other examples indicate the scientific and medical value of TCM, which is increasingly being recognized by the western world.
At present, a number of TCM methods and agents are being used to treat RA, with promising clinical efficacy. TCM herbal formulas developed by analyzing the personalized conditions of "when, where, and who” in individual patients have been shown to alleviate the symptoms of many patients with RA who fail to respond to chemical drugs. With the development and utilization of omics and bioinformatics in the field of TCM research, the scientific implication of an increasing number of herbal formulas has been elucidated, which has led to a better understanding and acceptance of TCM by western scientists [26]. Importantly, many compounds or ingredients extracted from medicinal herbs have been proven to exert anti-inflammatory and anti-arthritis effects in vitro and in vivo, with specific action targets that are somewhat different from the marketed chemical drugs. For example, ZhengQingFengTongNing (ZQFTN), a TCM patented drug containing a monomer chemical sinomenine (SIN) derived from the medicinal plant Caulis Sinomenii, was approved by the State Food and Drug Administration of China (rebranded and restructured as the China Food and Drug Administration (CFDA) in 2013, and now rebranded and restructured as the National Medical Products Administration of the State Administration for Market Regulation of PRC since 2018) 20 years ago as a treatment for RA and was recently accepted by the National Health Insurance Directory of China, due to its high clinical efficacy and low toxicity in treating RA [21]. In addition, Tripterygium wilfordii Tablets and Tripterygium Glycoside Tablets developed from the medicinal herb Tripterygium wilfordii exhibited similar efficacy to MTX as well as enhanced efficacy when a combined remedy of the tablets and MTX was administered to patients with RA in randomized controlled clinical trials [27,28]. With the increasing understanding of its efficacy and mechanism, TCM has a promising future with broad applications in China and around the world. In this review, we focus on advancements in TCM research and possible breakthroughs in the near future to promote the globalization of TCM as a treatment for RA.
《2. Treating RA based on the TCM theory of syndrome differentiation》
2. Treating RA based on the TCM theory of syndrome differentiation
《2.1. Rooted in traditional practice》
2.1. Rooted in traditional practice
RA has been well documented in ancient Chinese medical literature, which includes the treatment principle of syndrome differentiation of a patient with the disease. In the earliest Chinese medical classic, Huangdi Neijing (Inner Canon of Huangdi), RA was classified as "Bi syndrome”—also known as "HeXiFeng,” "LiJieFeng,” and so forth [29]—and was characterized by the obstruction of meridians and collaterals in the body. According to TCM theories, Bi syndrome is generally caused by wind, cold, and dampness, three major pathogenic factors contributing to RA. In other words, the basic etiology of RA is wind, cold, and dampness [26]. Based on these factors, RA is further divided into three subcategories [30]: "Xing Bi,” a syndrome affected by excessive wind that involves the mobility of the affected joints and variability of manifestations; "Tong Bi,” severe pain in the fixed joints and symptoms that worsens when the body is exposed to cold; and "Zhuo Bi,” an arthritic syndrome caused by excessive dampness [31]. Moreover, unless we can clarify the specific etiological factors in different stages of RA, we cannot provide corresponding therapies [32]. For example, in the later stage of Bi syndrome, the pathological products of phlegm and blood stasis block channels and collaterals and further extend to muscles and poly-joints, which may hinder recovery or increase susceptibility to recurrence [33,34]. In these circumstances, Chinese medicinal herbs with the effects of removing blood stasis and clearing phlegm-dampness should be added to the prescription to enhance therapeutic effectiveness. Thus, differential treatment strategies should be employed to treat RA according to the different TCM syndromes exhibited by individual patients.
As a major unique characteristic of TCM, combined therapy using an herbal formula based on syndrome differentiation has been advocated for approximately 1900 years. The first drug treatise in the earliest Chinese medicinal classics, Shennong Bencao Jing (Shennong’s Classic of Materia Medica), recorded that Aconitum Carmichaelii was used to treat patients who were affected by cold and dampness inducing knee pain or difficulty walking, such as ‘‘Tong Bi.” Dr. Zhongjing Zhang in the Eastern Han Dynasty established the classical TCM formulas WuTou Decoction (WTD) and GuiShaoZhiMu Decoction (GSZMD) as treatments for arthralgia [35,36]. At present, WTD exhibits similar therapeutic efficacy in treating cold-dampness RA to that of the chemical drug MTX [37]. Furthermore, the combination of WTD with MTX or leflunomide (LEF) achieves better clinical outcomes than the monotherapy of western medicine [38–40]. GSZMD has also been shown to have equal or superior effectiveness to chemical drugs in treating RA, with fewer adverse effects. According to a systematic review and meta-analysis of 13 randomized clinical trials (RCTs), treatment with GSZMD was more effective than treatment with standard protocols of western medicine, and only two studies reported adverse events associated with the GSZMD group [41]. These results highlight the value of classic formulas in treating RA according to the TCM theory of syndrome differentiation.
Other formulas, including DuHuoJiSheng Decoction (DHJSD), which was proposed by Dr. Simiao Sun in the Tang Dynasty, and DangGuiNianTong Decoction (DGNTD), which was established in the Qing Dynasty, are currently included in the National Health Insurance Directory of China [42]. DHJSD is suitable for relieving arthritic symptoms by strengthening the general physical conditions of older patients with RA [43], while DGNTD has been applied to treat Bi syndrome induced by dampness and heat with severe poly-joint swelling [44]. These published studies and clinical experiences indicate that the ancient TCM physicians identified a close correlation between specific TCM syndromes/patterns and the effective corresponding formula, which has in fact been verified many times by other physicians over hundreds or thousands of years. Although TCM theories and formulas are difficult to understand in contemporary scientific terms or lack scientific data to some degree, they have already provided us with valuable resources, and particularly with a strong experience-based clinical treatment for future studies of refractory cases of RA and in discovering ideal anti-arthritic and rheumatic agents.
《2.2. An integrated approach using traditional methods and modern technologies》
2.2. An integrated approach using traditional methods and modern technologies
At present, the use of syndrome differentiation to treat RA with TCM has not yet been well-unified, and related descriptions or records in the ancient TCM books and literature are limited. This situation has led to challenges in standardizing the use of TCM to diagnose and treat patients with RA, while modern technologies are required to elucidate the mechanistic explanations of TCM treatment [45,46]. In general, an herbal formula consists of several types of medicinal herbs or minerals, one of which may represent the principle component while others serve as adjuvant herbs to assist the principle herb in the therapeutic targeting of the illness and well-defined syndrome of a patient diagnosed with RA [47]. We hypothesize that, at least in some formulas, multiple active chemical components in one herbal formula trigger multiple molecular targets to exert synergistic therapeutic effects on RA. In addition, new technologies and methods should be used to extensively evaluate the therapeutic value, further improve the formulations, enhance the therapeutic efficacy, and reduce the adverse effects of some ancient formulas in a more scientific manner. Dissection of the mode of action of clinically well-established TCM formulas, such as the Realgar-Indigo naturalis formula (RIF), which has been proven to be very effective in treating humans with APL, is an excellent example of the application of both analytic and synthetic research approaches at the molecular, cellular, and organism levels [48]. Based on the molecular mechanisms, tetraarsenic tetrasulfide was determined to be the principle component of the RIF formula, with tanshinone and indirubin serving as adjuvant ingredients. This successful example encourages researchers to utilize multiple cutting-edge technologies for both basic and clinical studies of TCM formulas as treatments for RA, with a particular focus on revealing their composition and molecular mechanisms. WTD, which is one of the most effective formulas for patients with RA presenting with ‘‘Tong Bi” syndrome, contains Aconiti Radix (Ac), Ephedrae Herba (Ep), Paeoniae Radix Alba (Pa), Astragali Radix (As), and Glycyrrhizae Radix (Gl). The chief herb in WTD is Ac, without which the effective functions of WTD were shown to be significantly reduced in RA patients [37]; thus, Ac is called the emperor herb. However, Ac is also a toxic herb that may cause adverse clinical reactions, including severe arrhythmia and neurotoxicity if used improperly [49]. Therefore, in WTD, Ep and As, as the minister herbs, are used to enhance the antiarthritic effect of Ac, while Pa and Gl, as the assistant and servant herbs, respectively, are used to reduce the side effects of the emperor herb. In addition, WTD recommends decocting Ac for 1–2 h with honey to further reduce the toxicity of the aconitum alkaloids contained in Ac [50–54]. In fact, this formulation creates an effective synergy in treating refractory cases of RA (Fig. 1). According to the formulation principles in WTD, TCM doctors might modify ancient formulas to improve the formulation. In our previous study, GuanJieKang (GJK), a modified formula derived from WTD, exerted a significant protective effect on bone destruction in rats with experimental arthritis that was comparable to the effect of MTX but exerted fewer side effects than MTX and WTD [55].
《Fig. 1》

Fig. 1. The principal of the formulation of WTD. Ac represents the principal component (emperor), and other herbs serve as adjuvant herbal components to enhance therapeutic efficacy or reduce adverse effects. BAC: benzoylaconine; DDAs: diester-diterpenoid alkaloids.
When developing proper prescriptions of medicinal herbs, TCM doctors must accurately differentiate the syndromes of patients with RA. However, syndrome differentiation is a relatively subjective concept, and judgments of syndrome differentiation rely on the experience of TCM doctors [56]. Physicians must accurately analyze symptoms that may represent different stages of diseases in order to normalize and standardize syndrome differentiation; this is applicable to RA treatment, particularly when formulating appropriate treatment prescriptions in the context of personalized medicine [57,58]. A few efforts have been made to build a bridge between syndrome differentiation and the correlation of the serum biomarkers of RA. Recently, an analysis examined data from 10 articles including 77 healthy volunteers and 1150 patients with RA who were categorized as having cold, heat/hot, or deficiency syndrome, and reported a correlation between syndrome differentiation and serum biomarker levels [59]. The different types of TCM syndromes showed a diverse range of biomolecules, proteins, and genes in patients with RA that were well correlated with the cold, heat/hot, or deficiency phenotype-based TCM patterns. These identified biomarkers may hold potential to be further developed as diagnostic biomarkers for the early detection and monitoring of patients with RA [59]. These biomarkers would be useful to stratify subsets of patients with distinct biological bases, and might then help physicians—even young doctors or western doctors—choose the optimal biomedical therapy. Taken together, integrated approaches to treating RA with traditional methods and modern technologies are required in order to improve both our understanding of TCM syndrome differentiation and global TCM application.
《3. Advancement of TCM clinical studies in treating RA》
3. Advancement of TCM clinical studies in treating RA
《3.1. Major Chinese proprietary medicines derived from TCM formulas 》
3.1. Major Chinese proprietary medicines derived from TCM formulas
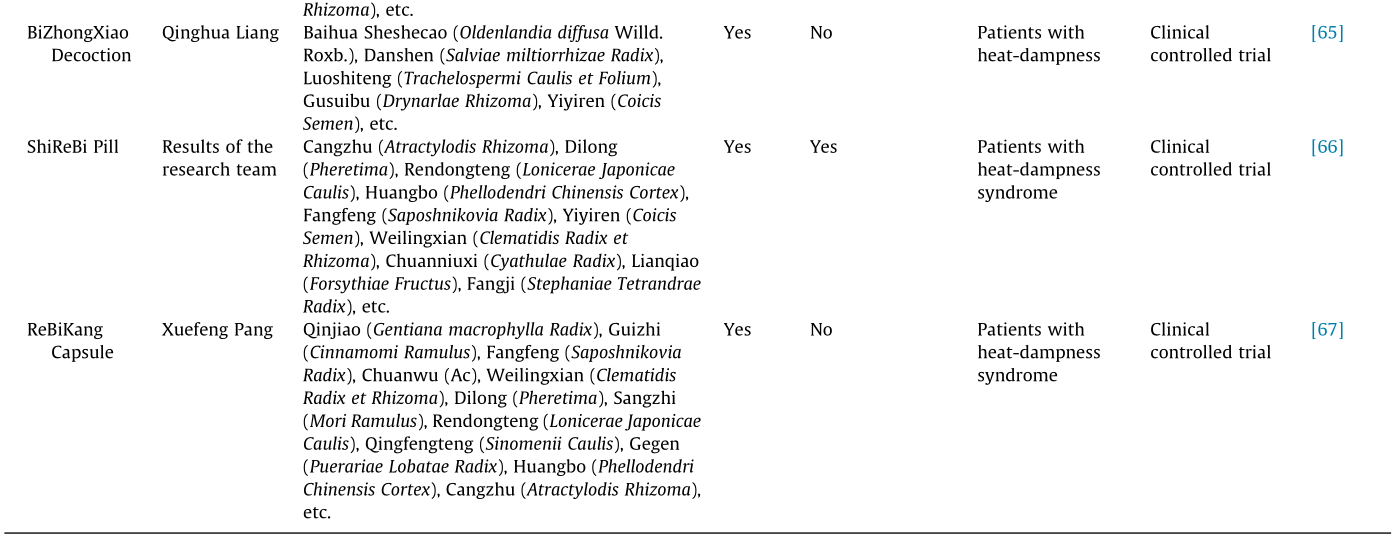
In addition to the classical formulas, TCM doctors themselves have optimized the classical formulas or developed their own formulas according to their clinical experience, some of which have been further developed into Chinese proprietary medicines (CPMs) according to the relevant guidelines of the CFDA and approved as treatments for RA. These CPMs exhibit clear indications and clinically therapeutic efficacies that are useful for all TCM and western medical doctors. Moreover, some CPMs are easily obtained in the medical markets and may conveniently be taken by patients with RA themselves. However, sufficient guidelines are not available for all CPMs regarding their optimal administration, particularly for patients treating themselves. Moreover, western medical doctors sometimes experience difficulty in properly prescribing CPMs according to the TCM syndrome differentiation theory when they have not yet been well trained in TCM. Another critical point of CPMs is a requirement for sufficient data from clinical trials, and particularly for RCTs or personalized pragmatic randomized controlled trials (PPRCTs), because such clinical trials provide direct evidence of the effectiveness, efficacy, and suitableness of the tested CPMs for individual patients with RA. Therefore, an increasing number of clinical trials have been performed in China in recent years. In 2017, dozens of CPMs were employed as RA treatments and resulted in good outcomes, according to the National Health Insurance Directory of China, such as BiQi Capsule, KunXian Capsule, YiShenJuanBi Pill, WangBi Electuary, TongBi Capsule, HanShiBi Pill, ShiReBi Pill, and more (Table 1) [42,60–67]. In addition, co-administration of BiQi Capsule with MTX resulted in higher efficacy than the monotherapy of BiQi Capsule or MTX, and this combined therapy reduced the side effects of MTX [60]. Based on the expert consensus in treating RA in China, YiShenJuanBi Pill and WangBi Electuary were recommended as treatments for patients with RA in the inactive stage, and have been listed in the guidelines since 2013 [42]. According to several clinical studies, YiShenJuanBi Pill markedly improves clinical symptoms and relieves bone erosion in patients with RA, and is particularly effective in patients with early-stage or age-related RA [68,69]. WangBi Electuary alleviates the symptoms of patients with RA in a relatively short time when combined with MTX, and the efficacy of this combined therapy has been shown to be better than the combined therapy of MTX and LEF [70]. TongBi Capsule and HanShiBi Pill are highly recommended for patients with RA presenting with cold-dampness syndrome. Moreover, TongBi Capsule has been used to treat age-related RA when combined with MTX, and shows better effectiveness and fewer side effects than the MTX monotherapy [62]. HanShiBi Pill is more suitable for long-term treatment courses because it exerts fewer gastrointestinal effects while simultaneously producing good effects on arthritis [63,64]. For patients diagnosed with heat-dampness syndrome, TCM doctors may select BiZhongXiao Decoction, ShiReBi Pill, or ReBiKang Capsule.
《Table 1》
Table 1 Major CPMs derived from TCM formulas as treatments for RA.

《3.2. Major CPMs derived from TCM monomers/ingredients》
3.2. Major CPMs derived from TCM monomers/ingredients
CPMs derived from TCM monomers/ingredients rank at the top of all CPMs for treating RA in China, and are frequently administered in combination with western chemical drugs to produce synergistic treatment results. Using analytical methods in natural pharmaceutical chemistry, many monomers or active ingredients with anti-inflammatory effects have been identified, such as Tripterygium wilfordii [71], SIN [72], paeoniflorin [73], artesunate [74], baicalin [75], calycosin [76], licochalcone A [77], dihydromyricetin (DMY) [78], sanguiin H-6 [79], curcumin [80], peony glucosides [81], and the ethanolic extract of Aralia continentalis Kitag. [82], among others. Of these formulations, Tripterygium Glycoside Tablets, ZQFTN Tablets, and Total Glucosides of Peony (TGP) Capsules have been widely used in China with substantial therapeutic efficacy (Table 2) [83–85]. Thus, patients with RA—and especially patients who are unable to tolerate the side effects or inefficacy of western chemical drugs—are offered a wide range of choices of agents for achieving remission of the disease.
《Table 2》
Table 2 Major CPMs derived from TCM monomers/ingredients as treatments for RA.

Tripterygium glycosides are the active ingredients extracted from Celastraceae Tripterygium wilfordii Hook. F. (TwHF) plants, which include a number of diterpenoids, alkaloids, and triterpenoids, and a few glycosides. The efficacy and safety of TwHF have been proven in several multi-center RCTs. In 2015, Lv et al. [86] conducted a multi-center, open-label RCT and revealed that the TwHF monotherapy was not inferior to—and that MTX + TwHF was better than—MTX monotherapy in controlling disease activity in patients with active RA. This finding attracted wide attention from the international community and was published in the Annals of the Rheumatic Diseases. By systematically reviewing data published before 2016, researchers also found that TwHF was more effective in improving the American College of Rheumatology (ACR) 20 response rate and the ACR 50 response rate compared with DMARDs. However, for patients in the child-bearing period, attention should be paid to the reproductive function when using TwHF to treat RA, as TwHF has been reported to exert adverse menstrual effects [83].
Since the 1990s, our research team has performed a series of studies on the anti-inflammatory and anti-arthritis effects of SIN [87]. In cooperation with the Hunan Zhengqing Pharmaceutical Group Co., Ltd., ZQFTN, a series of SIN preparations, was successfully developed. In an analysis of 956 patients with RA from 11 RCTs, the combination of ZQFTN with MTX improved the efficacy of the MTX monotherapy and was superior in terms of controlling adverse drug reactions [84]. Chinese clinicians from various areas have published 114 papers to evaluate the therapeutic efficacy of ZQFTN on 5566 cases, with a reported efficacy of 85.2%. Interestingly, in contrast to non-steroidal anti-inflammatory drugs (NSAIDs), almost no cardiovascular side effects were reported following the administration of ZQFTN in the clinic, which indicates that ZQFTN exerts distinct effects from the existing cyclooxygenase (COX)-2 inhibitors [88].
TGP Capsules have also been approved as a disease-modifying oral drug for RA by the State Food and Drug Administration of China since 1998. A systematic review of eight RCTs enrolling 1209 patients with active RA was conducted in 2017 [85], and the results showed that TGP might be an appropriate choice as an adjuvant therapy with DMARDs for patients with RA, as improvements in the ACR 20 response rate, ACR 50 response rate, and ACR 70 response rate, along with fewer adverse effects, were observed [85]. However, unlike TwHF and ZQFTN, TGP exerts relatively mild effects on RA. Therefore, TGP seems to be more suitable for patients with inactive RA.
TwHF, ZQFTN, and TGP have been widely accepted in China as treatments to enhance the effectiveness and reduce the toxicity of DMARDs in patients with RA. Therefore, a rational option is to administer MTX together with TCM in a combination therapy for patients in the early stages of RA. Moreover, ZQFTN and TGP are suitable for most patients with RA at any stage, and few side effects have been reported to date; thus, these two CPMs are highly recommended as basic medications or long-term maintenance medications for patients with RA.
《4. Characteristics and scientific foundations of using TCM to treat RA》
4. Characteristics and scientific foundations of using TCM to treat RA
《4.1. Differences in the therapeutic mechanisms of TCM and chemical drugs》
4.1. Differences in the therapeutic mechanisms of TCM and chemical drugs
The properties of chemicals derived from Chinese medicinal herbs may differ from those of synthesized chemical drugs. Moreover, multiple active components must be present in a Chinese herbal formula that exerts synergistic therapeutic effects on diseases via multiple drug-action targets and pathways, or through compound–compound interactions. Therefore, we anticipate that researchers will identify bioactive compounds, ingredients, or mixtures from natural sources to further develop them into natural products or drugs to treat human diseases. In fact, this strategy has been proven to be a successful alternative for drug discovery alongside the pharmaceutical industry of synthesized chemical drugs. The structure of NSAIDs consists of an acidic moiety attached to a planar, aromatic functional group [89], and the primary molecular target of these drugs is COXs, which are required for the metabolism of cell membrane-derived arachidonic acid (AA) to form pro-inflammatory prostaglandins [90]. Therefore, NSAIDs exhibit strong potency in suppressing prostaglandin E2 (PGE2) synthesis and subsequently significantly relieving inflammation and pain. However, NSAIDs may decrease prostacyclin (PGI) activity by inhibiting COX-2 and then upset the balance between PGI and thromboxane (TX), as well as inhibiting the inflammatory mediator PGE2, leading to cardiovascular events, which are one of the major side effects of NSAIDs. In addition, patients with RA frequently experience chronic poly-joint pain and inflammation, which may require long-term treatment or even life-long pain management, while the dominant property of NSAIDs is to relieve acute pain [91].
SIN is an alkaloid that is structurally similar to morphine but does not cause addiction. Importantly, unlike COX inhibitors, SIN not only inhibits the activation of immune-related cells and the secretion of pro-inflammatory cytokines, but also selectively restrains the synthesis of membrane-bound prostaglandin E syntha-1 (mPGES-1), an enzyme involved in the last step of PGE2 synthesis. In other words, SIN directly targets mPGES-1 to inhibit PGE2 synthesis, but does not interfere with the balance between PGI and TX, thus avoiding cardiovascular side effects. Although mPGES-1 is a promising target for drug discovery, no drug has yet been developed for the global market. Thus, ZQFTN, which includes SIN, is the first drug available to treat RA by inhibiting mPEGS-1 [88]. Moreover, SIN exerts a significant protective effect on bone that is comparable to that of MTX by rebuilding the balance between matrix metalloproteinases (MMPs) and tissue inhibitors of metalloproteinase (TIMP); thus, SIN is not only an antiinflammatory drug, but also a natural DMARD that improves disease prognosis [92] (Fig. 2).
《Fig. 2》
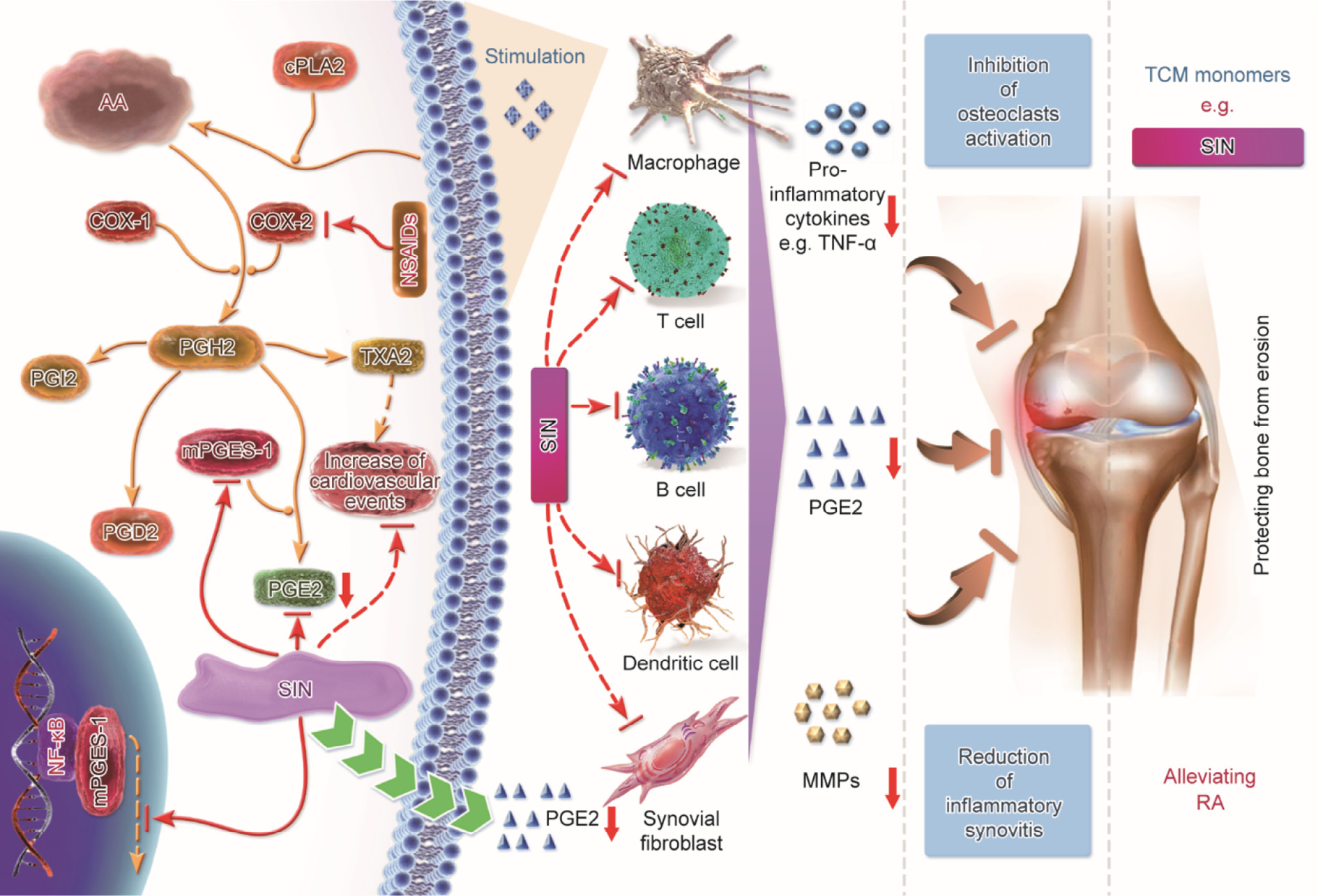
Fig. 2. The molecular mechanism by which SIN treats RA. cPLA2: cytosolic phospholipase A2; PGD2: prostaglandin D2; PGH2: prostaglandin H2; PGI2: prostaglandin I2; TXA2: thromboxane A2; NF- : nuclear factor kappa B.
: nuclear factor kappa B.
Flavonoids are the most abundant phenolic compounds exhibiting anti-oxidant, anti-inflammatory, and immunomodulatory properties [93,94]. Many bioactive flavonoids, such as licochalcone, baicalein, and puerarin, have powerful anti-inflammatory effects. Therefore, flavonoids are another potential category of natural chemicals for the discovery of anti-inflammatory and antiarthritis drugs. For example, DMY, a type of flavonoid isolated from Ampelopsis grossedentata (Hand.-Mazz.) W.T. Wang, suppresses  kinase β (IKK-β)–nuclear factor kappa B (NF-) signaling, T cell activation, and cytokine production in purified human T lymphocytes; more interestingly, its anti-inflammatory effect on IKKbC46A mice is diminished. DMY covalently binds the Cys-46 binding site of IKK-β kinase, which suggests that Cys-46 is a novel drugbinding site for the inhibition of IKK-β, and drug-resistant patients with the IKK-β mutant genotype might eventually be treated with this new IKK-b inhibitor [78]. Thus, TCM is a great treasure trove of biomedical resources for the discovery of novel drugs for use in China and around the world. In addition to the specific effective targets, the network-based regulation of holism is a unique medical system in TCM, unlike chemical drugs.
kinase β (IKK-β)–nuclear factor kappa B (NF-) signaling, T cell activation, and cytokine production in purified human T lymphocytes; more interestingly, its anti-inflammatory effect on IKKbC46A mice is diminished. DMY covalently binds the Cys-46 binding site of IKK-β kinase, which suggests that Cys-46 is a novel drugbinding site for the inhibition of IKK-β, and drug-resistant patients with the IKK-β mutant genotype might eventually be treated with this new IKK-b inhibitor [78]. Thus, TCM is a great treasure trove of biomedical resources for the discovery of novel drugs for use in China and around the world. In addition to the specific effective targets, the network-based regulation of holism is a unique medical system in TCM, unlike chemical drugs.
《4.2. Network-based drug action of TCM in treating RA》
4.2. Network-based drug action of TCM in treating RA
With the rapid development of multi-omics technologies, the methods for understanding the mechanisms of drug actions have rapidly changed from single-target action to multiple-targets actions. In our previous studies, capsules of QingFuGuanJieShu (QFGJS) were found to significantly inhibit experimental arthritis and acute inflammation by reducing the production of proinflammatory cytokines and increasing the production of antiinflammatory cytokines [95]. Using two-dimensional (2D) gels and matrix-assisted laser desorption/ionization time-of-flight mass spectrum/mass spectrum (MALDI-TOF-MS/MS), the antiarthritis effects of QFGJS were proven to be mainly related to 14 proteins; among these, the Pgk1 protein was found to play a central role in modulating metabolism, which provides substantial support for the use of a combined remedy containing the Chinese herbal formula as a treatment for arthritis [95]. In addition, 18 biomarkers were identified from serum samples of subjects treated with HuangLianJieDu Decoction using the collagen-induced arthritis model, and these biomarkers were found to participate in several metabolic pathways [96]. Moreover, this formula was also found to reverse the progression of RA by partially regulating the metabolism of fatty acids and AA. Berberine (BBR), a major component in Rhizoma Coptidis (Huanglian), was also confirmed to treat RA by modulating fatty acid and cholesterol synthesis pathways; however, its anti-arthritic effect is largely blocked by the addition of intermediate metabolites in these two pathways [97]. Based on these results, the modulation of metabolism at the cellular and organ levels is a crucial mechanism by which TCM treats RA [98].
Since TCM combinations might generally produce local or systemic effects on the digestive tract following oral administration, the intestinal micro-ecology must exert a mediating effect during treatment. The composition and function of the intestinal flora are crucial indexes reflecting the holistic concept of TCM combinations. For example, polysaccharides in Astragalus membranaceus and lotus plumule resolve into short chain fatty acids to further perform their anti-arthritic and anti-inflammatory functions[99,100]. Gene-sequencing techniques could be used to further validate and analyze the correlations between changes in the intestinal flora and therapeutic indicators of TCM combinations to reveal their anti-arthritic actions. As shown in our recent study, GJK, a Chinese medicinal formula in which five herbs are modified, significantly relieves the symptoms of arthritis and prevents bone erosion in rat models of arthritis. This drug also reverses the imbalance in the intestinal flora, which is closely correlated with the improvement in inflammatory cytokine production and the mechanism of bone protection. Thus, a correlation analysis of macro-genomics based on the intestinal microflora is very important for explaining the holistic regulatory mechanism of TCM and predicting potential targets for RA treatment [98].
In addition, systematic approaches using multi-omics technologies may provide novel insights into medical and pharmaceutical studies, particularly studies aiming to elucidate the complicated molecular mechanisms of multiple components contained in an herbal formula exhibiting multi-target characteristics. For example, GSZMD, a classical herbal formula used to treat RA, comprises nine Chinese herbs containing 637 chemicals [101], while a functional analysis of GSZMD found that 1327 targets of these 637 chemicals may be involved in many biological networks that mediate drug actions. The therapeutic effect of GSZMD may result from regulation of the Fc epsilon RI signaling pathway, the adipocytokine signaling pathway, and lipid metabolism, which are closely associated with mediator release, inflammatory pathologies, antigen-driven autoimmune responses, whole-body lipid metabolism, and matrix degradation in human joints. An investigation of 10 inferred gene clusters from expression profiles with a target association network revealed that the GSZMDspecific targets directly or indirectly interacted with disease genes that are essential for immune-associated biological processes[101]. Furthermore, histone deacetylase (HDAC)1–heat shock protein (HSP)90AA1–NF-2–IKK-β–TNF-α was the dominant signaling pathway contributing to the therapeutic efficacy of the formula [36]. Therefore, the complicated mechanism of GSZMD was gradually elucidated by employing a three-step strategy: discovering the targets, conducting network analysis, and confirming by experimental validation. Similarly, target prediction and network analysis of WTD revealed that its anti-arthritic action is closely associated with the regulation of the macrophage CCR5 signaling pathway [35]. Together, a network-based approach using multi-omics technologies is a valuable strategy for elucidating the complicated molecular mechanisms of Chinese herbal formulas, and can allow researchers not only to uncover the mysteries of TCM in a scientific manner, but also to push forward treatment with drug combinations into the new area of the pharmaceutical industry, particularly as cures for refractory human illnesses [102].
《5. Perspectives》
5. Perspectives
Over the past two decades, substantial advances have resulted in the expansion of TCM from China to the world; however, researchers must still strive to achieve breakthroughs in TCM research in order to enable it to become a world-class treatment in mainstream international markets and to be accepted by mainstream medicine. Integrated approaches in the early diagnosis and treatment of RA with TCM, the identification of effective new therapeutics with a clear demonstration of drug-action targets and mechanisms, and intensive RCTs or PPRCTs that adhere to international standards are required to achieve these goals (Fig. 3).
《Fig. 3》

Fig. 3. Perspectives for studies of TCM: advancing TCM from empirical practice to evidence-based therapy. MALDI-TOF/TOF MS: matrix-assisted laser desorption/ionization time-of-flight/time-of-flight mass spectrometry; PGC: porous graphitic carbon.
《5.1. Early diagnosis and early treatment》
5.1. Early diagnosis and early treatment
Identifying RA at the initial presentation and treating patients with drugs that display few side effects can affect the disease course, prevent the development of joint erosions, or delay the progression of erosive disease [103,104]. Early diagnosis and treatment are particularly important for patients who will develop a more serious disease. Recently, the capacity of artificial intelligence (AI) to diagnose or predict disease risk has been developing rapidly [105]. For example, researchers have revealed AI models that scan retinal images to predict eye and cardiovascular disease risks. We postulate that AI diagnostics are likely to improve the therapeutic delivery and effectiveness of RA as computing power and the neural networks that underlie deep learning are improved. Moreover, AI systems have been created to analyze data, notes, and reports from a patient’s file, external research, and clinical expertise in order to guide clinicians in selecting the correct, individually customized treatment path—including TCM—at an early stage. However, AI diagnostics or treatments are not yet ready for the clinic. Many researchers in the field complain that too many developers are not extending the studies far enough; for example, there is an insufficiency of biomarkers for early diagnosis and treatments in the database [106]. Therefore, integrating research with innovative RA biomarker discovery is very important. Our previous work revealed the importance of sulfated IgG N-glycans in the prediction and diagnosis of RA. A new microfluidic TiO2–porous graphitic carbon (PGC) chip was developed for in-depth glycomic research of antibody glycosylation patterns, and new functional sulfated glycans were first identified as potentially useful tools for differentiating between RA, ankylosing spondylitis, and osteoarthritis diagnoses [107]. Interestingly, researchers have confirmed that aberrant IgG galactosylation is a dysregulated component of the humoral immune response in patients with RA that begins prior to disease onset and is associated with disease activity in a sexspecific manner; this finding indicates that IgG N-glycans are potential biomarkers for the early diagnosis of RA [108]. However, the specific disease biomarkers for RA at an early stage are still insufficient, and there would be a great demand for effective and safe drugs, particularly drugs treating RA at an early stage. TCM drugs, which display comparable effectiveness and fewer side effects than DMARDs, are the potential first choice for patients with early-stage RA.
《5.2. Precise diagnosis and personalized treatment》
5.2. Precise diagnosis and personalized treatment
Personalized treatment is particularly important for patients with RA. Approximately one-third of patients do not respond to a specific biological therapy because the course of RA is highly multifaceted [109]. Further clinical studies on RA are expected to identify disease-specific genes, proteins, or metabolites in large-scale evaluations, which rely on the analysis of big data and on information provided by several omics fields that have been developed in the last few decades: genomics, transcriptomics, proteomics, epigenomics, microbiomics, and exposomics. Omics technologies are high-throughput techniques that enable researchers to gather large amounts of data about a specific type of molecule—such as the three billion base pairs of the human genome, the universe of proteins in a given tissue, or a large collection of metabolites—in a single experiment. Examples of these technologies are nextgeneration sequencing, which is used for genomics and transcriptomics studies, and autoflex speed MALDI-TOF/TOF MS, which is used for proteomics. TCM is characterized by a personalized and holistic approach [110], and TCM doctors are often able to identify multiple signs and symptoms and then summarize them into a unique syndrome/pattern to guide the treatment of each individual patient. This practice remains a mainstay of empirical practice. Therefore, the transformation of the principles of TCM into a systems biology approach using multi-omics technologies would enable the establishment of a new TCM system with precise diagnosis and treatment, as well as predictive and preventive health management within a framework of personalized medicine [102].
《5.3. Discovery of new drugs》
5.3. Discovery of new drugs
TCM is an important treasure trove for developing novel targeted anti-arthritis drugs. The use of computational simulations and virtual coupling between small molecules derived from TCM and disease-specific proteins could help researchers to avoid random drug selection. Moreover, stem cell and three-dimensional (3D) printing techniques could be used to achieve in vitro models that reproduce the course of disease progression and facilitate the discovery of key proteins or targets associated with RA pathology [111,112]. Thus, the application of computational modulation techniques, including molecular docking, might increase the success rate and accuracy in the process of selecting a drug from the TCM composition database, which would make significant contributions to drug discovery [113]. The etiology and pathogenesis of RA are complicated, and may involve various targets and signaling pathways with diverse pharmacological drug actions. Therefore, strategies exploiting different effective compositions to modulate those targets and signaling pathways might produce more effective results than a single composition. For this purpose, a meaningful approach is to extract effective components from TCM formulas in order to develop new drugs to treat diseases. In addition, the identification of novel multi-target agents acting on multiple domains, including proteins, lipids, and amino acids, is valuable for the discovery of drugs to treat RA.
《5.4. Evidence from vast clinical trials》
5.4. Evidence from vast clinical trials
Most TCM doctors are currently treating RA in an empirical manner, which places severe restrictions on the use of TCM and results in low acceptance of TCM RA treatment worldwide. In these circumstances, high-quality RCTs are particularly required to conduct an array of high-quality basic studies designed to establish a new TCM system with evidence-based therapies for treating RA. In addition, PPRCTs designed to assess TCM effectiveness with highly personalized clinical protocols are expected to be adopted [114]. We should also set priorities in TCM research for treating RA by developing a strategic plan, which may include designing standard multi-center large-sample RCTs or PPRCTs; confirming the effects, safety, and characteristics of different CPMs; and establishing international collaborative efforts with international standards in all basic and clinical studies. Moreover, quality control of pharmaceutical preparations containing TCM formulas with quality markers should be ensured when clinical trials are conducted [115,116].
Overall, TCM is a treasure trove for researchers, and transforming the use of TCM from empirical practice to evidence-based therapy is the most critical task facing clinical researchers in this field. These studies will ensure the sustainable development of TCM in a vital, beneficial, and contributable way for humankind in the future.
《Acknowledgements》
Acknowledgements
The authors thank Prof. Boli Zhang, an academician of Chinese Academy of Engineering, for his valuable advice and suggestions to undertake this review. This work was financially supported by the grants from the Macao Science and Technology Development Fund (102/2016/A3, 0032/2018/AFJ).
《Compliance with ethics guidelines》
Compliance with ethics guidelines
Hu-Dan Pan, Yao Xiao, Wan-Ying Wang, Ru-Tong Ren, Elaine Lai-Han Leung, and Liang Liu declare that they have no conflict of interest or financial conflicts to disclose.
《Nomenclature》
Nomenclature
AA arachidonic acid
Ac Aconiti Radix
ACR American College of Rheumatology
AI artificial intelligence
APL acute promyelocytic leukemia
As Astragali Radix
AS ankylosing spondylitis
As2O3 arsenic trioxide
ATRA all-trans retinoic acid
BAC benzoylaconine
BBR berberine
CFDA China Food and Drug Administration
COX cyclooxygenase
cPLA2 cytosolic phospholipase A2
CPM Chinese proprietary medicine
DDA diester-diterpenoid alkaloid
DMARD disease-modifying anti-rheumatic drug
DHJSD DuHuoJiSheng Decoction
DGNTD DangGuiNianTong Decoction
DDA diester diterpenoid alkaloid
DMY dihydromyricetin
Ep Ephedrae Herba
GSZMD GuiShaoZhiMu Decoction
GJK GuanJieKang
Gl Glycyrrhizae Radix
HDAC histone deacetylase
HSP heat shock protein
IKK-β I kinase β
LEF leflunomide
MTX methotrexate
mPGES-1 membrane-bound prostaglandin E syntha-1
MMP matrix metalloproteinase
MALDI-TOFMS/MS matrix-assisted laser desorption/ionization timeof-flight mass spectrum/mass spectrum
MALDI-TOF/ TOF MS matrix-assisted laser desorption/ionization timeof-flight/time-of-flight mass spectrometry
NF- nuclear factor kappa B
NSAID non-steroidal anti-inflammatory drug
Pa Paeoniae Radix Alba
PGC porous graphitic carbon
PGE2 prostaglandin E2
PGD2 prostaglandin D2
PGH2 prostaglandin H2
PGI prostacyclin
PGI2 prostaglandin I2
PPRCT personalized pragmatic randomized controlled trial
QFGJS QingFuGuanJieShu
RA rheumatoid arthritis
RCT randomized clinical trial
RIF Realgar-Indigo naturalis formula
SIN sinomenine
TCM traditional Chinese medicine
TNF tumor necrosis factor
TB tuberculosis
TGP total glucosides of peony
TwHF Tripterygium wilfordii Hook. F.
TIMP tissue inhibitors of metalloproteinase
TXA2 thromboxane A2
WTD WuTou Decoction
ZQFTN ZhengQingFengTongNing











 京公网安备 11010502051620号
京公网安备 11010502051620号




