
《1 Introduction》
1 Introduction
Discipline classification and specialties catalogues serve as guidance for and cornerstones of discipline advancement, department setting, and teaching. Complete, scientific classification of disciplines and specialties is an important foundation for the development of world first-class disciplines in higher education institutions in China. The specialties catalogues of China’s higher education institutions, based on discipline characteristics and research fields, are divided into three levels: the Higher Vocational Education Specialties Catalogue (Junior Colleges) in Higher Education (2015) (hereinafter referred to as the higher vocational specialties catalogue); the Undergraduate Specialties Catalogue in Higher Education (2012) (hereinafter referred to as the undergraduate specialties catalogue); and the Catalogue of Degree Awarding and Talent Training (2011) for Master’s/Doctoral Education (hereinafter referred to as the master’s/doctoral specialties catalogue). The three specialties catalogue levels have played a positive role in the standardization and promotion of higher education in China. However, these three levels represent separate systems and lack coordination with one another, and parts of the catalogues are outdated and fail to capture the essence of the characteristics of higher education [1].
Within the field of medicine, clinical medicine is a highly practical discipline. Medical education also involves lengthy training, high degree requirements, and rapid updating of knowledge. The changing situation and challenges of global health have led to the setting of new goals and directions for the advancement of medicine; meanwhile, medical education is undergoing a new round of revolution worldwide, which inevitably demands new modules and curricula [2–3]. Proper understanding of the nature of education and organization of specialties catalogues is highly significant to the fostering of excellence in disciplines and the cultivation of outstanding medical professionals [4]. This research focused on medical specialties catalogues in China, the United States, and the UK, conducted a comparative study of the classification and characteristics of medical specialties in these three countries, determined deficiencies in medical specialty definition in China, and proposed reform proposals.
《2 Status quo of global medical specialties catalogues》
2 Status quo of global medical specialties catalogues
《2.1 Overview of discipline and specialty definition》
2.1 Overview of discipline and specialty definition
China’s specialties catalogue is formulated by the Ministry of Education. It classifies higher vocational education into 19 discipline groups, 99 disciplines, and 748 specialties, and undergraduate education into 12 discipline groups, 92 disciplines, and 506 specialties. The classification of master’s/doctoral education has been adjusted four times, and currently, there are 13 discipline groups, 110 first-level disciplines, and 386 second-level disciplines.
The management system of disciplines and specialties in the United States is quite mature, and there is a relatively complete classification system of disciplines and specialties. Government administrators, members of medical associations, and university administrators jointly participate in the formulation of the Classification of Instructional Programs (CIP). The final version of CIP is proposed by the National Center for Education Statistics (NCES) and officially promulgated by the Department of Education (ED). The current CIP (CIP-2000) was finalized in April 2002 and applies to graduate, undergraduate, and vocational education. There are a total of 38 discipline groups and 362 disciplines, and specialties in each discipline are dynamically adjusted [5–7].
Higher education institutions in the UK set majors and curricula based on teaching capacity and societal demand, and discipline and the definition of disciplines and specialties has its own system. In 2002, the British Higher Education Statistics Agency (HESA) and the Universities and Colleges Admissions Service (UCAS) jointly proposed the Joint Academic Coding System (JASC), a discipline and specialties catalogue with general applicability, which has been revised twice in 2007 and 2012 [8–9].
《2.2 Definition of medical disciplines》
2.2 Definition of medical disciplines
China’s higher vocational education catalogue defines the Medicine and Health discipline as comprising eight first-level disciplines: Clinical Medicine, Nursing, Pharmacy, Medical Technology, Rehabilitation Treatment, Public Health and Management, Population and Family Planning, and Health Management and Promotion. Under the umbrella of these disciplines are 46 specialties (including state-controlled specialties).
China’s undergraduate education catalogue defines the Medicine discipline as comprising11first-level disciplines: Basic Medicine, Clinical Medicine, Stomatology, Public Health and Preventive Medicine, Traditional Chinese Medicine, Integrated Chinese and Western medicine, Pharmacy, Chinese Materia Medica, Forensic Medicine, Medical Technology, and Nursing. Under the umbrella of these disciplines are 44 specialties (including specialties established for specific purposes).
China’s master’s/doctoral education catalogue defines the Medicine discipline as comprising11 first-level disciplines: Basic Medicine, Clinical Medicine, Stomatology, Public Health and Preventive Medicine, Traditional Chinese Medicine, Integrated Traditional Chinese and Western Medicine, Pharmacy, Chinese Materia Medica, Medicine in Specific Environments, Medical Technology, and Nursing. Under the umbrella of these disciplines are 54 second-level disciplines. Moreover, an education catalogue for professional degree is set in specialties such as Clinical Medicine, Stomatology, Public Health, Nursing, Pharmacy, Chinese Materia Medica.
In the US CIP-2000, Health Professions and Related Clinical Sciences comprise 34 disciplines (excluding disciplines in Biological and Biomedical Sciences) and 207 specialties. Medical subject areas in the British JACS3.0 are mainly distributed among Medicine and Dentistry and subjects allied with Medicine. There are 15 first-level disciplines and 78 specialties.
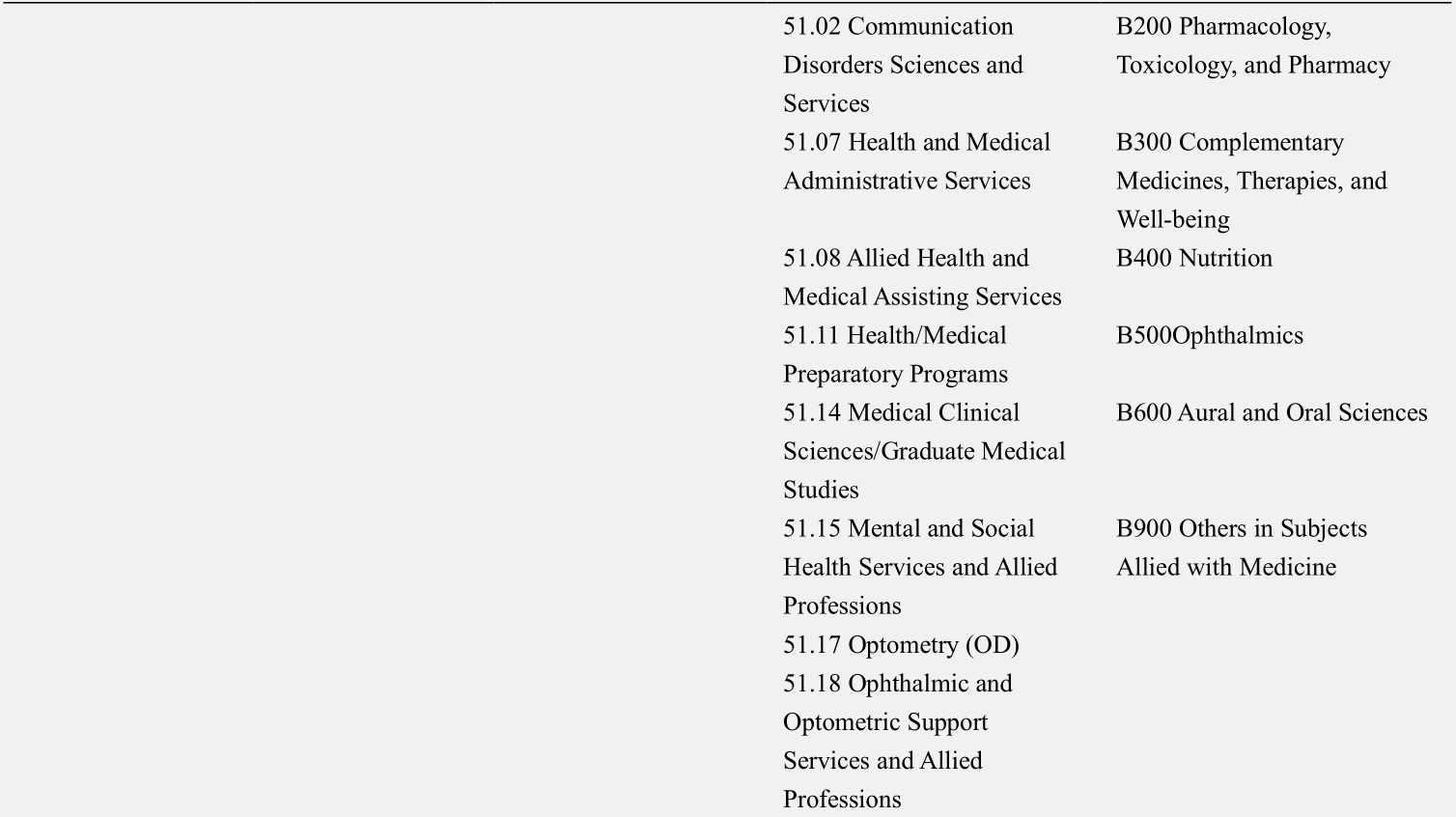
In comparison (Table 1), the number of medical disciplines in China is low. In terms of disciplines, the United States and the UK have additionally developed Allied Health and Medical Assisting Services, Communication Disorders Sciences and Services, Medical Clinical Sciences, Medical Ethics, Ophthalmology, and Nutrition, among others. However, there are no similar definitions in China’s three-level educational catalogue (first-level disciplines).
《Table 1》
Table 1. Comparison of medical discipline and specialty definition (first-level disciplines) in China, the United States, and UK.





《2.3 Definition of specialties in clinical medicine》
2.3 Definition of specialties in clinical medicine
In China, a clinical medicine discipline is defined in the higher vocational education catalogue. The undergraduate catalogue defines the clinical medicine discipline (core discipline) and anesthesiology, medical imaging, ophthalmology, psychiatry, radiology, and other disciplines for specific purposes and state-controlled disciplines. There are 18 specialties in the master’s/doctoral clinical medicine catalogue, including internal medicine, pediatrics, geriatric medicine, and neurology, among others.
Conversely, in developed countries, represented by the United States and the UK, there are no second-level disciplines in clinical medicin eor premature sub-classifications of specialties in medical education. The secondlevel disciplines of clinical medicine in the graduate education catalogue in China are comparable to medical specialties in post-graduate training in the United States. Table 2 lists the second-level disciplines in clinical medicine.
《Table 2》
Table 2.Comparison of medical disciplines and specialty definition (second-level disciplines) in China, the United States, and the UK.


Note : T, K separately stand for specialties for specific purposes and state-controlled specialties.
*Family Medicine was newly defined in 2012 by the Office of the State Council Academic Degrees Committee.
《2 Problems with defining medical specialties catalogues in China》
2 Problems with defining medical specialties catalogues in China
《2.1 Catalogues are not uniform》
2.1 Catalogues are not uniform
China’s higher vocational, undergraduate, and master’s/doctoral education all define their specialties catalogues separately, leading to poor coordination between the three levels and deterioration of the overall planning and scientific development of higher education in China. By contrast, the United States and the UK each define a single catalogue across all stages of medical education, covering the full range. For example, the CIP-2000 (United States) has a corresponding, consistent, and coordinated subject catalogue for graduate, undergraduate, and vocational education.
《2.2 Lags in content and quantity in catalogues》
2.2 Lags in content and quantity in catalogues
Modern medicine is evolving rapidly, and the number of disciplines and sub-disciplines is expanding significantly and is more interconnected. The shift from a “biomedical” to a “biological–psychological–social” paradigm and changes in the disease spectrum require that doctors possess humanistic qualities and comprehensive competencies beyond professionalism in knowledge and skills. However, the current specialties catalogues do not reflect many of these interdisciplinary aspects or cutting-edge medicine and the medical paradigm shift. Proposals to define specialties such as medical humanities are not considered important or popularized, which could potentially impede the development of medicine and the cultivation of medical professionals in China.
In terms of the number of specialties, there are 34 disciplines and 207 specialties in medicine in the United States, while the range of medical disciplines and specialties in China is relatively small. There are only 11 disciplines and 54 specialties in master’s/doctoral-level medical education. In terms of the range of disciplines, China’s definitions lack humanity and interdisciplinary features among disciplines such as Allied Health and Medical Assisting Services, Communication Disorders Sciences and Services, Medical Clinical Sciences, and Medical Ethics.
《2.3 Clinical medicine is prematurely subdivided and specialized》
2.3 Clinical medicine is prematurely subdivided and specialized
The clinical medicine discipline is a field with broad coverage. The United States and the UK define the clinical medicine program only as medical school, rather than as pediatrics, psychiatry, or preventive medicine. In general, education in medical school should cover a broad range of disciplines. Doctors can only diagnose in their specific specialties after first gaining a general background in medical practice and systematic knowledge of human life and health. However, China’s current specialty definitions in master’s/doctoral medical education are prematurely subdivided, as 18 sub-specialties have been defined in clinical medicine. This leads medical students to develop narrow clinical knowledge, with less adaptability in practice, degrading the outcomes of medical education.
《2.4 The master’s/doctoral medical specialties catalogue is not coordinated with the residential training specialties catalogue》
2.4 The master’s/doctoral medical specialties catalogue is not coordinated with the residential training specialties catalogue
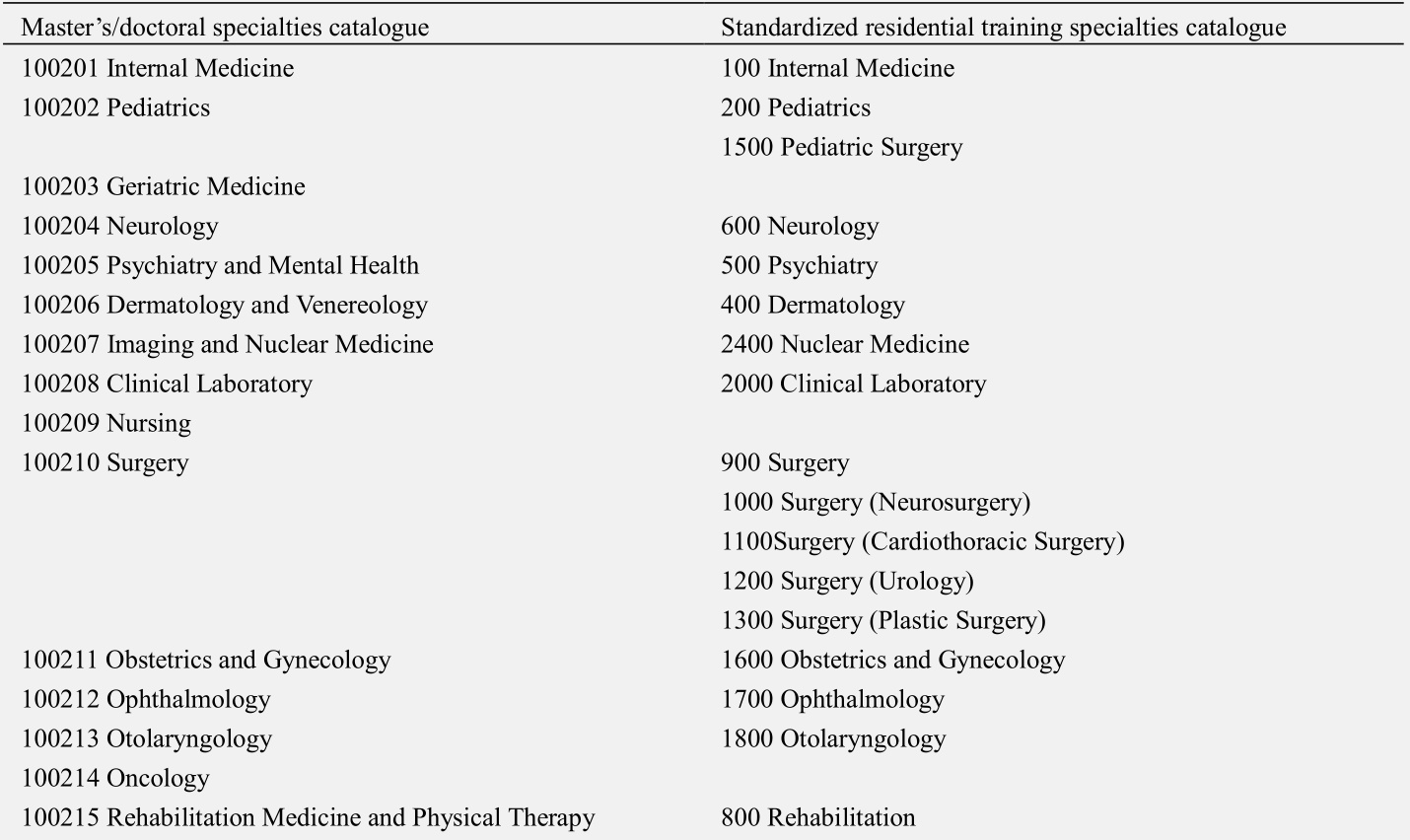
After completing education in medical school, the medical student begins post-graduate training. At present, China’s graduate medical education (professional track) coexists with standardized residential training, and specialty definitions are disproportionate (Table 3), which results in many contradictions and problems in the training process. Sorting out the specialties catalogues to be coordinated should be prioritized for improvement.
《Table 3.》
Table 3. Comparison of medical specialties definition in master’s/doctoral education and standardized residential training in China.

《3 Suggestions for defining medical catalogues in China》
3 Suggestions for defining medical catalogues in China
《3.1 Medical specialties definition should be based on the current situation and gradually aligned with global standards.》
3.1 Medical specialties definition should be based on the current situation and gradually aligned with global standards.
To address incompatibilities between China’s medical specialties definition and international standards, it is suggested that specialties definition be based on the national situation and international experiences. Then, our medical specialties definition should be gradually synchronized with advances in modern medicine and aligned with internationally accepted medical specialties catalogues.
First, a unified specialties catalogue should be established. The specialties catalogue definition practices of CIP (United States) and JACS (UK), among others, could be consulted for the overall planning of specialty definition for different discipline levels and to ensure the logicality and continuity of medical specialties catalogues at the junior college, undergraduate, and graduate education phases and provide smooth coordination that is conducive to the overall development of higher education in China.
Second, medical specialties catalogues should be updated dynamically. Based on demands of social development and international experiences in defining emergent and interdisciplinary aspects of disciplines, it is suggested to optimize the catalogues by defining new specialties such as Allied Health and Medical Assisting Services, Communication Disorders Sciences and Services, Medical Clinical Sciences, Medical Ethics, and so on.
Third, the discipline system should be enriched to match international standards. For example, currently, the medical discipline of pharmacy in China comprises only: Medicinal Chemistry, Pharmaceutics, Pharmacognosy, Pharmaceutical Analysis, Microbiology and Biochemical Pharmacy, Pharmacology, and so on. Specialties such as Pharmacoeconomics, Pharmacy Management, and Pharmacy Policy should also be established to enrich the pharmacy discipline in China.
《3.2 Establishing a standardized mechanism of inclusion and exclusion among medical specialties》
3.2 Establishing a standardized mechanism of inclusion and exclusion among medical specialties
The establishment of a scientific and standardized mechanism of inclusion and exclusion among medical specialties in China is conducive to the standardized management of discipline and specialty definition and the proper updating, adjustment, and long-term development of disciplines and majors. It is suggested that a dynamic updating mechanism for medical specialties be established and adjusted every five years, according to the Degree Awarding and Talent Training Specialty Catalogue Definition and Management Measures. Thus, the catalogue would represent the opinions of stakeholders and enable educational institutions to achieve greater autonomy. Moreover, this would allow government, society, and universities to unleash their potential in the definition and management of specialties catalogues [10].
《3.3 Medical specialties catalogues should be cohesive and coordinated.》
3.3 Medical specialties catalogues should be cohesive and coordinated.
Medical education, as a comprehensive and multi-level educational system, must obtain a unified set of specialties catalogues with clarity across different phases. Moreover, teaching priorities should be clearly emphasized in undergraduate and graduate studies, to prevent misalignment and inefficiency in medical education [1].Clinical medicine in medical school, especially, features a wide range of specialties, and this premature subdivision and specialization is inappropriate and can affect the growth of medical talents. Furthermore, the definition of clinical medicine specialties catalogues should not only be coordinated within undergraduate and graduate studies but also consider coordination with specialties catalogues of standardized residential training. Through joint efforts of medical schools and hospitals, a continuum of education could be provided to medical students, so that they can transition smoothly, in an orderly manner, from graduate medical studies to post-graduate medical training, which is conducive to the cultivation of qualified and standardized medical talents.











 京公网安备 11010502051620号
京公网安备 11010502051620号




