
《1. Introduction》
1. Introduction
Over the past decades, Doppler echocardiography has gained a wide range of clinical applications in the early detection, severity quantification, therapeutic decision-making, and prognostic estimation of a variety of cardiovascular diseases [1]. However, standardization of Doppler echocardiography has received less attention than M-mode and two-dimensional echocardiography (2DE). As yet, no international guidelines have recommended normal reference values for Doppler echocardiography, whereas cutoff values for M-mode and 2DE parameters were recommended by the American Society of Echocardiography (ASE) and the European Association of Echocardiography as early as 15 years ago [2]. This omission was largely due to the lack of reliable and systemic normal reference values for Doppler echocardiography in adults until the recent publications of several large, prospective, and multicenter studies, such as the Normal Reference Ranges for Echocardiography (NORRE), the Echocardiographic Measurements in Normal Chinese Adults (EMINCA), and the Japanese Normal Values for Echocardiographic Measurements Project (JAMP) [3–5]. A major finding in these studies was that most Doppler values vary considerably with age and gender, resulting in a wide dispersion of Doppler measurements in healthy subjects and making it difficult to determine a cutoff threshold between normal and abnormal values. Among the many factors that may induce variations of Doppler measurements in healthy subjects, physiological variances induced by gender, age, height, weight, and heart rate may play an important role, and thus should be corrected using an appropriate method. Although Z scores have been used to normalize Doppler measurements for growth in children [6,7], they are obviously not suitable for mature adults.
Recently, we developed and verified an optimized multivariable allometric model (OMAM) for the correction of 2DE parameters in a healthy Chinese Han population [8]. As left ventricular (LV) function is determined by its structure, the gender differences in LV Doppler measurements are likely attributable to differences in body size. In addition, it is known that heart rate may affect some Doppler measurements. Therefore, the aims of the present study were to: ① verify the hypothesis that different LV Doppler measurements correlate nonlinearly with different biometric variables raised to different scaling factors and exponents; ② establish scaling equations using the OMAM for the correction of LV Doppler parameters; ③ establish reference standards for normality for OMAM-corrected LV Doppler parameters; ④ assess the applicability of the OMAM in overweight subjects; and ⑤ correct LV Doppler parameters using a single-variable isometric model (SVIM) as a comparison.
《2. Methods》
2. Methods
《2.1. Study population》
2.1. Study population
As we reported in the EMINCA studies [4,9], a total of 1394 healthy Chinese Han adult volunteers were enrolled from 43 collaborating laboratories. Commercially available instruments— namely, the Philips iE33 (Philips Ultrasound, USA) or the GE Vivid E9 (GE Vingmed Ultrasound, Norway)—were used for the study. In an attempt to standardize echocardiographic image acquisitions and measurements, one or two experienced sonographers from each of the participating laboratories received intensive training at two core laboratories (Qilu Hospital of Shandong University and Sichuan Provincial People’s Hospital) to become acquainted with the study protocol and to obtain standard images and measurements in accordance with the ASE and European Association of Cardiovascular Imaging (EACVI) guidelines [1,10]. All the LV Doppler parameters were measured by two experienced sonographers in the two core laboratories.
Since the purpose of this study was to remove the physiological effects of biometric variables and to establish reference standards for normality for OMAM-corrected LV Doppler parameters, we chose 1224 subjects with a body mass index (BMI) below 25.0 kg·m–2 for mathematical and statistical analyses in order to avoid the potential pathological effects of overweightness and obesity on the allometric equations. In order to establish a reliable and stable correction model, the subjects were randomly assigned into two groups: group A (70%, n = 857) to develop OMAM equations for the 23 LV Doppler parameters, and group B (30%, n = 367) to test the reliability of the OMAM equations. The applicability of the OMAM equations was also tested in 183 overweight subjects (BMI = 25.0–29.9 kg·m–2 ) without known cardiovascular diseases (group C).
The research protocol was approved by each Ethics Committee of all collaborating centers. Written informed consent was obtained from all subjects. The EMINCA study was registered (ChiCTR-OCS-12002119) at the Chinese Clinical Trial Registryy , an authorized organization of the International Clinical Trial Registr↑ Platform of the World Health Organization.
↑ http://www. chictr.org
《2.2. Mathematical and statistical analyses》
2.2. Mathematical and statistical analyses
To develop OMAM equations for LV Doppler parameters, we respectively plotted the relations between the uncorrected value (Yu) of each LV Doppler parameter and age (Age), height (H), weight (W), and heart rate (HR) in group A, and found that most of the LV Doppler measurements correlated nonlinearly with Age, H, W, and/or HR. We assumed that the relationship between the predicted value of each LV Doppler parameter (Yp) and the biometric variables of Age, H, W, and HR follows an exponential equation: Yp =  ·Agew·Hx ·Wy ·HRz , where a is the allometric scaling constant, and w, x, y, and z are the exponents of the independent variables Age, H, W, and HR, respectively. Since there were significant differences between men and women in 14/23 (60.9%) of the LV Doppler parameters in groups A and B before correction, we introduced gender into the above equation as a dummy variable, together with other biometric variables in group A, and found no significant effect of gender on Yp values after introducing age, height, weight, and heart rate into the OMAM. This finding suggested that the gender effect on Doppler measurements was mainly caused by the difference in body size variables between men and women. Since both BMI and body surface area (BSA) are calculated from height and weight using fixed exponential formulas, we did not introduce BMI and BSA as independent variables into the OMAM equations to avoid confounding interactions with the original values of height and weight.
·Agew·Hx ·Wy ·HRz , where a is the allometric scaling constant, and w, x, y, and z are the exponents of the independent variables Age, H, W, and HR, respectively. Since there were significant differences between men and women in 14/23 (60.9%) of the LV Doppler parameters in groups A and B before correction, we introduced gender into the above equation as a dummy variable, together with other biometric variables in group A, and found no significant effect of gender on Yp values after introducing age, height, weight, and heart rate into the OMAM. This finding suggested that the gender effect on Doppler measurements was mainly caused by the difference in body size variables between men and women. Since both BMI and body surface area (BSA) are calculated from height and weight using fixed exponential formulas, we did not introduce BMI and BSA as independent variables into the OMAM equations to avoid confounding interactions with the original values of height and weight.
By performing logarithmic transformation on both sides of the equation, the above exponential equation was transformed into a linear equation to facilitate linear regression analysis: Ln(Yp) = Ln() + w·Ln(Age) + x·Ln(H) + y·Ln(W) + z·Ln(HR). Then a stepwise multivariable linear regression analysis was performed to determine which variable(s) among Age, H, W, and HR could enter the formula and to derive the corresponding values of the scaling constant and the exponents w, x, y, and z for each of the individual LV Doppler parameters. Finally, the value of Yp was calculated by sub-stituting the values of , w, x, y, and z into the initial exponential formula Yp = ·Agew·Hx ·Wy ·HRz , and the corrected value (Yc) of each Doppler parameter was defined as a ratio of Yu to Yp as: Yc = Yu/Yp [8,11]. The traditional SVIM was also performed in 1224 subjects by dividing Yu by BSA, which was calculated by the Du Bois’ formula [12] and Yc was calculated as: Yc = Yu/BSA.
The reliability of the OMAM equations established in group A was then tested in both groups B and C. The corrected values of the LV Doppler parameters were calculated, and their correlations with uncorrected values and biometric variables were respectively analyzed using the bivariable Pearson correlation test. Theoretically, an ideal correction of Doppler measurements for physiological variances should satisfy two conditions [8,11]: First, the corrected Doppler values should be independent of age, height, weight, and heart rate, as all the effects of biometric variables with statistical significance were taken into account in the OMAM equations; and second, the correlations between the corrected and uncorrected values should remain significant, because variations in Doppler measurements induced by physiological variances account for only a small proportion of uncorrected Doppler values. Accordingly, we set strict criteria for successful correction: ① the absence of significant statistically and biologically residual correlations (r > 0.20 or (r < 0.20, P < 0.05) between the corrected values and each of the biometric variables; and ② the maintenance of significant correlations (P < 0.05) between the corrected and uncorrected values.
The normality of the distribution of the Doppler variables was assessed using the Kolmogorov–Smirnov test. Data were expressed as mean ± standard deviation (SD). Bivariate Pearson correlation analyses were used to compare corrected and uncorrected values, and to compare corrected values and biometric variables. The independent samples unpaired t-test was used to analyze the differences between genders for both uncorrected and corrected values. All statistical analyses were carried out by SPSS 23.0 statistical software (SPSS, Inc., USA), and a two-tailed P < 0.05 was considered to be statistically significant.
《3. Results》
3. Results
The demographic characteristics of the study population are listed in Table 1 and Table S1 in Appendix A. There were no significant differences in age, body size variables, blood pressure, or heart rate between groups A and B (all P > 0.05). The mean value of the BMI in group C was (26.3 ± 1.2) kg·m–2 (25.0–29.7 kg·m–2). The height, weight, BMI, BSA, and blood pressures in group C were significantly higher than those in group A (all P < 0.01). The uncorrected and corrected Doppler measurements were all normally distributed.
《Table 1》
Table 1 Demographic characteristics of the subjects in groups A and B.

Data were expressed as mean ± SD. SBP: systolic blood pressure; DBP: diastolic blood pressure; bpm: beats per minute. 1 mmHg = 133.3 Pa.
《3.1. Development of the OMAM equations in group A》
3.1. Development of the OMAM equations in group A
As listed in Table 2, different LV Doppler parameters in group A correlated allometrically with one or more of the biometric variable(s) with different scaling constants and exponents. Concretely, of the 23 LV Doppler parameters, six parameters correlated allometrically with age, height, and weight; six parameters with age and heart rate; three parameters with age, height, weight, and heart rate; two parameters with age, height, and heart rate; two parameters with age and height; one parameter with height and heart rate; one with age, weight, and heart rate; one with age only; and one with heart rate only.
《3.2. Verification of the OMAM equations in group B》
3.2. Verification of the OMAM equations in group B
As shown in Table 2, by applying the OMAM equations to group B, there were significant correlations between the corrected and uncorrected values for all 23 LV Doppler parameters (r = 0.680– 0.989, P < 0.001). In contrast, the residual correlations between the corrected values and each of the biometric variables were statistically (P < 0.05) and biologically (r > 0.20 or r < 0.20) significant for none of the 23 parameters. Thus, the success rate of the OMAM correction was 100% in group B according to the criteria. In addition, the coefficients of variation of the corrected values decreased significantly compared with those of the uncorrected values in group B (23.8% ± 4.6% vs 25.9% ± 5.8%, P < 0.001, Table S2 in Appendix A). As expected, all the mean values of the OMAM-corrected Doppler measurements were close to 1.0.
《Table 2》
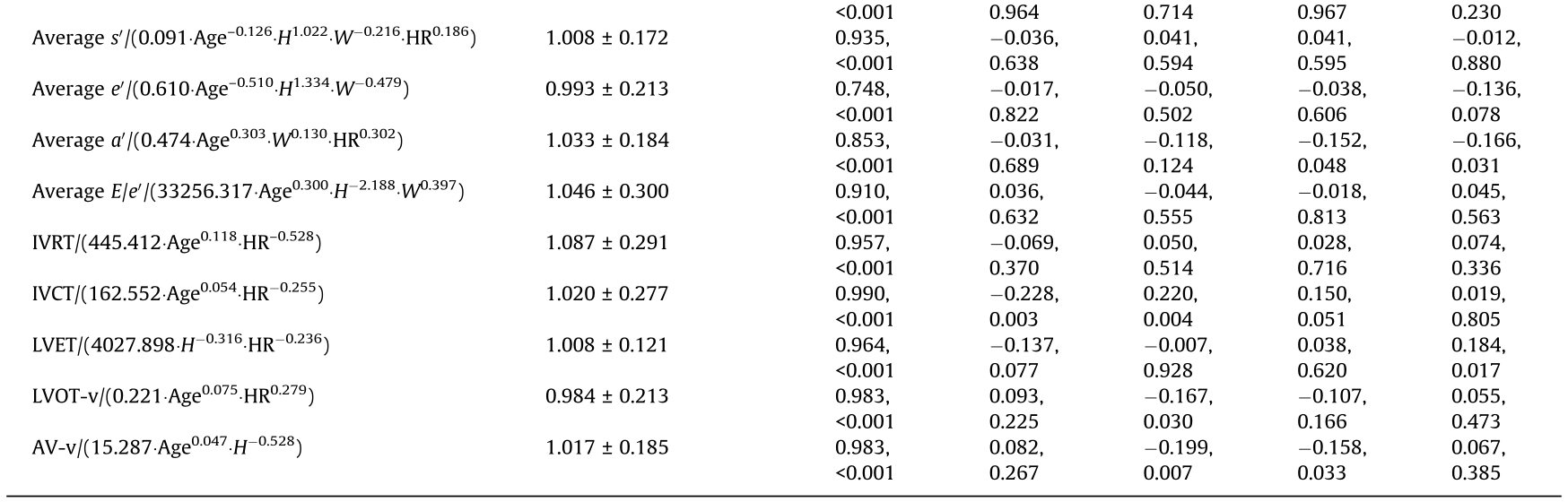
Table 2 OMAM equations developed in group A and validations in group B.
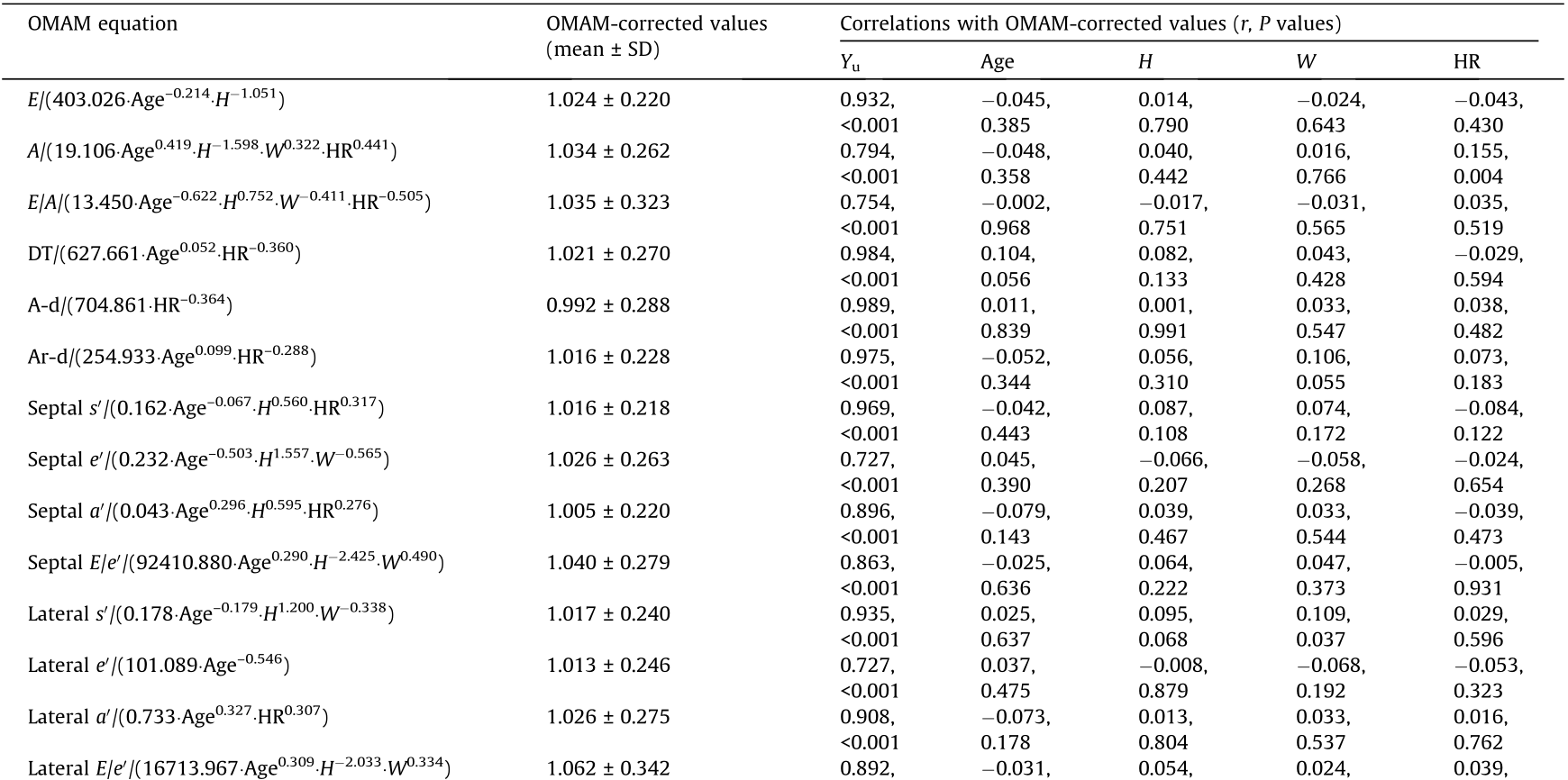
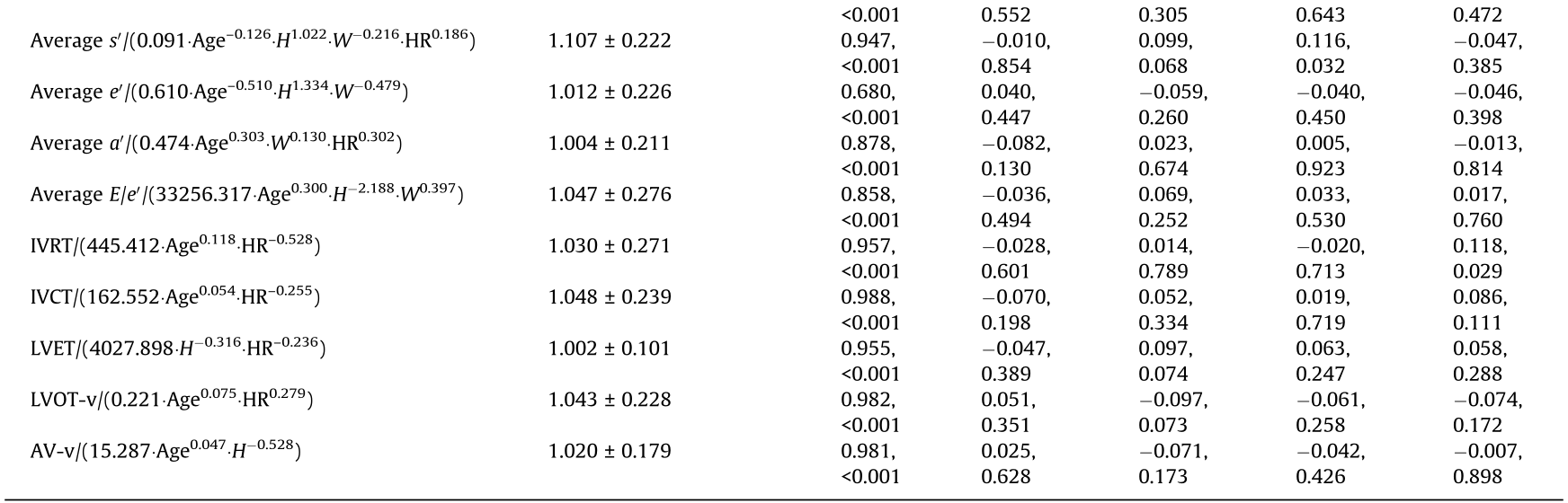
E: peak velocity of early diastolic mitral inflow; A: peak velocity of late diastolic mitral inflow; E/A: ratio of peak velocities of early to late diastolic mitral inflow; DT: deceleration time of E wave; A-d: time duration of late diastolic mitral inflow; Ar-d: time duration of atrial reversal wave from right upper pulmonary venous; s' : systolic velocity of mitral annulus; e' : early diastolic velocity of mitral annulus; a' : late diastolic velocity of mitral annulus; E/e' : ratio of early diastolic velocities of mitral inflow to mitral annulus; IVRT: isovolumetric relaxation time; IVCT: isovolumetric contraction time; LVET: left ventricular ejection time; LVOT-v: peak systolic flow velocity of left ventricular outflow tract; AV-v: peak systolic flow velocity of aortic valve.
《3.3. Effects of OMAM correction on gender differences in Doppler measurements》
3.3. Effects of OMAM correction on gender differences in Doppler measurements
All the uncorrected and OMAM-corrected Doppler values were normally distributed. In group B, there were significant gender differences in 11/23 (47.8%) of the uncorrected parameters (all P < 0.05). After correction using the OMAM equations, the gender differences were completely removed in 9/11 (81.8%) of the parameters, except for the lateral and averaged systolic velocities of mitral annulus, in which the absolute gender differences of the corrected values were very small (Table 3).
《Table 3》
Table 3 Gender differences in uncorrected and OMAM-corrected values of Doppler parameters in group B.

《3.4. Application of the OMAM equations in the overweight group》
3.4. Application of the OMAM equations in the overweight group
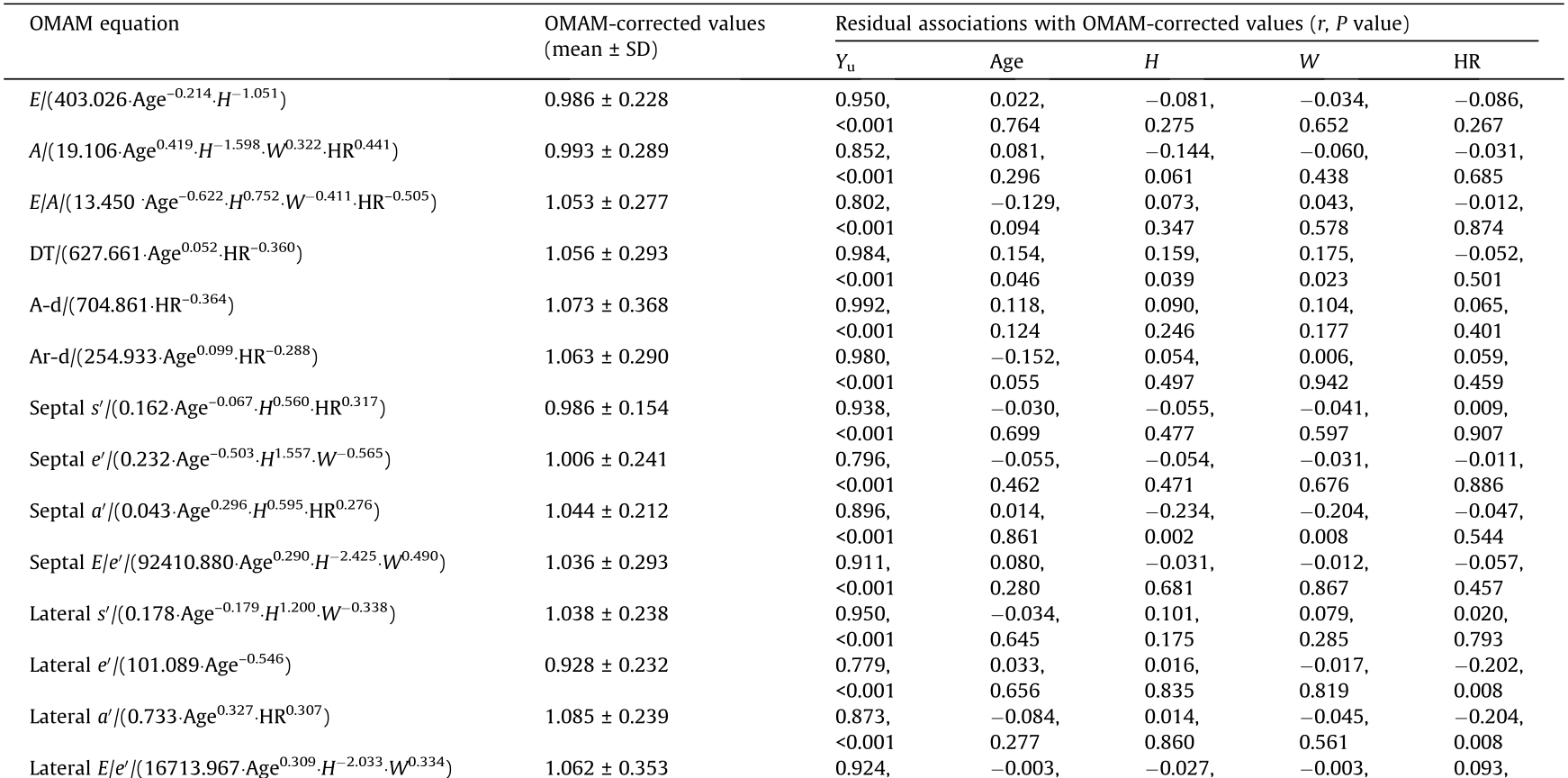
As shown in Table 4, the OMAM-corrected values correlated significantly with the uncorrected values of all 23 LV Doppler parameters (r = 0.748–0.992, P < 0.001). The residual correlations between the corrected values and one or more of the biometric variables were both statistically (P < 0.05) and biologically significant (r > 0.20 or r < –0.20) for four Doppler parameters. Therefore, the success rate of OMAM correction in the overweight group was 82.6% (19/23).
《Table 4》
Table 4 Applications of OMAM equations in group C.
《3.5. The SVIM with BSA as the sole scaling variable》
3.5. The SVIM with BSA as the sole scaling variable
As listed in Table S3 in Appendix A, before correction, all 23 LV Doppler parameters correlated significantly with one or more of the biometric variable(s). After correction using the SVIM with BSA as the single independent variable, there remained statistically and biologically significant residual correlations between the corrected values and the biometric variables in all 23 parameters; thus, the success rate of correction was zero. Notably, the absolute values of the correlation coefficients between the 23 BSA-corrected values and the BSA itself all increased in comparison with those before correction, suggesting that the use of the SVIM with BSA resulted in over-correction. Taking the ratio of peak velocities of early to late diastolic mitral inflow (E/A) and the average ratio of early diastolic velocities of mitral inflow to mitral annulus (E/e' ) as examples, the uncorrected values of E/A and average E/e' correlated significantly with age (Figs. 1(a) and (b)). By using the SVIM with BSA as a scaling variable, the corrected E/A and average E/e' values (E/A-SVIM and average E/e' -SVIM) still correlated significantly with age (Figs. 1(c) and (d)). Correction by the OMAM successfully eliminated the correlations between the corrected E/A and average E/e' values (E/A-OMAM and average E/e' -OMAM) and age (Figs. 1(e) and (f)).
《Fig. 1》
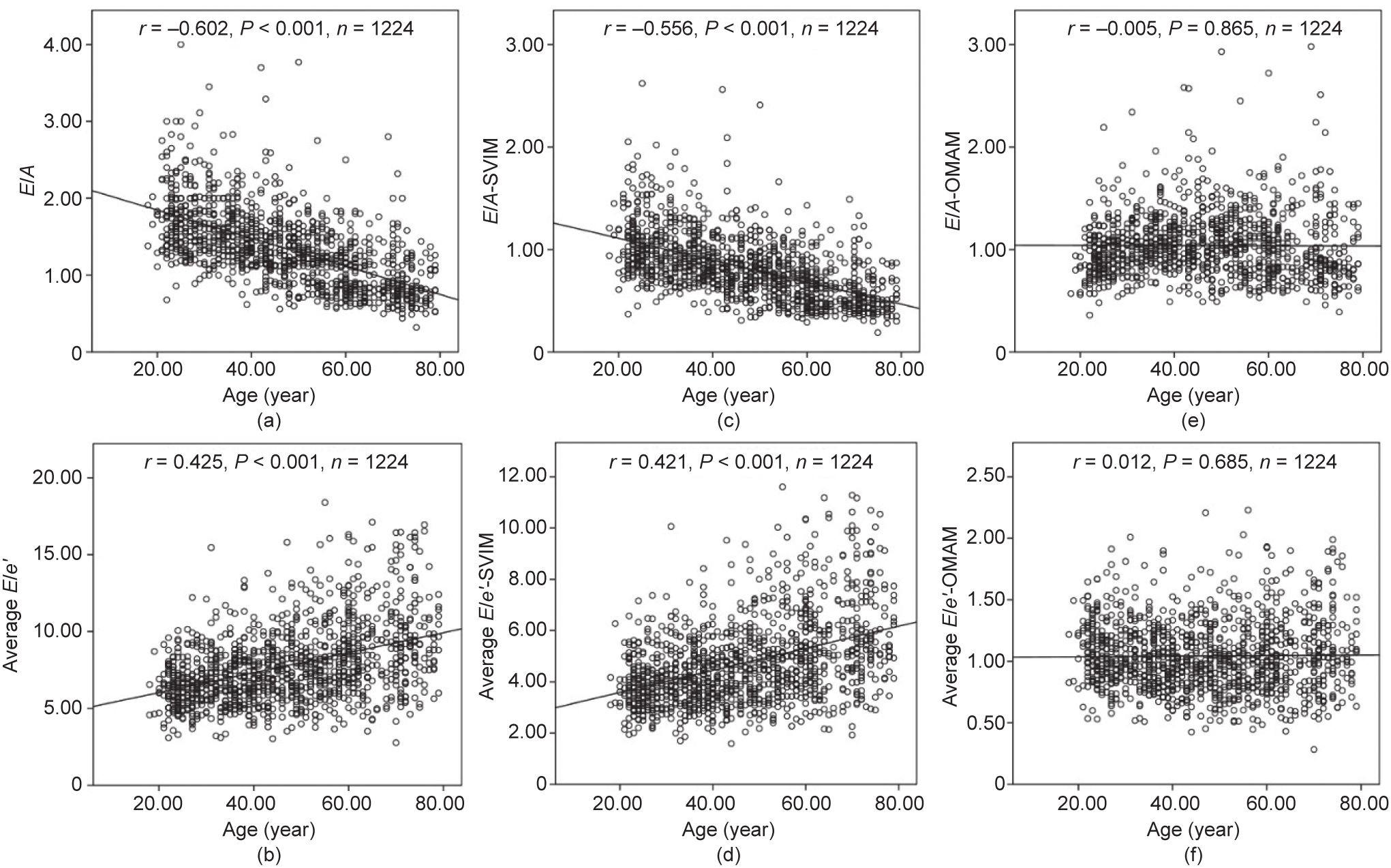
Fig. 1. Correlation analyses between values of E/A and average E/e' (uncorrected, SVIM-corrected, and OMAM-corrected) and age. (a) The uncorrected value of E/A correlated significantly and negatively with age (r = –0.602, P < 0.001); (b) the uncorrected value of average E/e' correlated significantly with age (r = 0.425, P < 0.001); (c) the correlation of the SVIM-corrected (with BSA as the scaling variable) value of E/A (E/A-SVIM) with age remained significant and negative (r = –0.556, P < 0.001); (d) the correlation of the SVIM-corrected (with BSA as the scaling variable) value of average E/e' (E/e' -SVIM) with age remained significant (r = 0.421, P < 0.001); (e) the OMAM-corrected value of E/A showed no residual correlation with age (r = –0.005, P = 0.865); (f) the OMAM-corrected value of average E/e' exhibited no residual correlation with age (r = 0.012, P = 0.685).
《4. Discussion》
4. Discussion
In this study, a total of 23 LV Doppler parameters were analyzed in 1224 healthy subjects, and most of the parameters were found to correlate allometrically with age, height, weight, or heart rate raised to different scaling factors and exponents. We set up a series of correction equations using the OMAM in 70% of the study population and verified their reliability in the remaining 30% of the subjects, as well as in an overweight group, with high success rates of correction. Corrected reference standards for normality were finally established for the 23 LV Doppler parameters. As far as we know, this is the first research to develop and validate a novel mathematical model for correcting LV Doppler parameters in an adult population.
《4.1. Correction of Doppler echocardiographic parameters》
4.1. Correction of Doppler echocardiographic parameters
Although it has been over six decades since the advent of Doppler echocardiography [13] studies on the correction of Doppler measurements for physiological variances have been limited to pediatric subjects, and the methodology derived from children is obviously not applicable to adults [6,7,14]. In most of these pediatric studies, the SVIM is commonly used as a scaling approach based on the arbitrary assumption that cardiac variables are linearly correlated to body size [15]. As both height and weight are integrated into the Du Bois’ formula [12] for the estimation of BSA, BSA has long been deemed the most appropriate body size variable for scaling cardiovascular measurements. In the present study, the use of the SVIM with BSA as the sole single variable resulted in increased residual correlation coefficients between the BSA-corrected values and BSA itself, suggesting an overcorrection in all 23 LV parameters, with a success rate of correction of 0. Thus, BSA is not an ideal variable for correcting the physiological variances of LV Doppler parameters.
In the current study, we first proposed a novel hypothesis: that the relationships between LV Doppler parameters and biometric variables follow a multivariable exponential equation in a healthy adult population. The results demonstrated that different LV Doppler parameters correlated allometrically to one or more of the different biometric variable(s) with different scaling constants and exponents, and the success rate of OMAM correction by our judging criteria for 23 LV Doppler parameters was 100%.
《4.2. Effects of biometric variables on the OMAM》
4.2. Effects of biometric variables on the OMAM
Previous studies in healthy adult populations have demonstrated the effects of age and gender on both blood flow and tissue Doppler measurements [3–5,16]. In our recently reported EMINCA study [4] over 40% and 80% of blood flow Doppler measurements and over 55% and 85% of tissue Doppler measurements differed significantly with different gender and age groups, respectively. An important finding of the present study was that resting heart rate correlated with more than half of the LV Doppler measurements, indicating that heart rate regulates hemodynamic changes. Therefore, we introduced age, height, weight, heart rate, and gender into the multivariable allometric model to remove the physiological effects of these variables on Doppler values. We found that gender failed to enter the model after other biometric variables had been introduced into the model, suggesting that the effect of gender on the uncorrected measurements was mainly attributed to the gender difference in body size. With this novel approach, the gender differences in 11 uncorrected parameters were completely removed in nine (81.8%) parameters with very small absolute gender differences for the remaining two corrected tissue Doppler measurements. A possible explanation for the dispersion in measured tissue Doppler velocities may be that different ultrasound instruments were used in the different participating centers in our study. This was further confirmed in a recent study showing remarkable discrepancies in ventricular myocardial velocities and myocardial time intervals that were measured by pulsed-wave Doppler tissue-imaging techniques designed by three different vendors [17].
To assess the efficacy of the OMAM in overweight subjects, we applied the OMAM equations to a group of 183 overweight individuals without known cardiovascular abnormalities and found that the success rate of correction decreased to 82.6% (19/23). The residual correlations between the biometric variables and the corrected values of septal  , lateral e' , lateral , and isovolumetric contraction time (IVCT) were slightly beyond our criteria for successful correction, and the possibility of vendor-induced differences cannot be completely excluded. These results suggested that overweightness did induce an adverse effect on the OMAM equations, albeit not dramatically so. Further studies in obese populations are necessary to identify the pathological effect of obesity on Doppler measurements after removing the effects of physiological weight variance and other biometric variables in individuals.
, lateral e' , lateral , and isovolumetric contraction time (IVCT) were slightly beyond our criteria for successful correction, and the possibility of vendor-induced differences cannot be completely excluded. These results suggested that overweightness did induce an adverse effect on the OMAM equations, albeit not dramatically so. Further studies in obese populations are necessary to identify the pathological effect of obesity on Doppler measurements after removing the effects of physiological weight variance and other biometric variables in individuals.
《4.3. Normal reference values of the corrected Doppler parameters》
4.3. Normal reference values of the corrected Doppler parameters
To avoid the potential interference of overweightness and obesity on the allometric scaling equations, we did not include overweight and obese subjects in the correction model. We developed the OMAM equations in Chinese healthy adults with a BMI below 25.0 kg·m–2 and set up the corrected reference values for 23 LV Doppler parameters, which can be used to replace the age- and gender-specific reference values in routine clinical practice. Taking average E/e' as an example and by referring to the method of Kuznetsova et al. [18] the cutoff values for an abnormally increased average E/e' (mean + 1.96SD) were 8.89, 10.32, 10.91, 11.99, 12.93, and 14.18 for men, and 9.80, 11.02, 11.91, 13.08, 15.44, and 16.72 for women in the age groups of 18–29, 30–39, 40–49, 50–59, 60–69, and 70–79 years, respectively, in this study. For a given value of the measured average E/e' in a given subject, it is necessary to compare it with the cutoff values in his/her corresponding gender and age group to ascertain whether this subject has LV diastolic dysfunction. In contrast, using the current OMAM equation with all physiological variances incurring to the average E/e' values eliminated, the cutoff value for the abnormally increased OMAMcorrected average E/e' (mean + 1.96SD) is 1.598. For a given value of the measured average E/e' in a given subject, it is only necessary to introduce the subject’s age, height, and weight into the OMAM equation specific for the average E/e' in Table 2 to calculate the corrected value for the average E/e' . By comparing the corrected value with 1.598, it is immediately clear whether or not LV diastolic dysfunction exists. In comparison, our OMAM is not only simple and reliable for case diagnosis, but also helpful for establishing a universal diagnostic criterion in a population.
《4.4. Study limitations》
4.4. Study limitations
This study contained some limitations. First, in order to avoid the effects of different ethnicities on the normal reference values of the corrected Doppler parameters, we included only healthy Chinese Han adults in the study population. Whether our OMAM equations are equally applicable to Western adults is therefore an open question. Recently, the World Alliance Societies of Echocardiography (WASE) normal value study revealed a significant inter-country variation in LV dimensions, mass, and volumes, even after indexing to BSA, and suggested that not only gender and age, but also nationality should be taken into account for defining the ranges of normality [19]. Thus, whether the OMAM can eliminate the physiological variances induced by different ethnicities awaits further investigation. Second, since we did not include obese subjects in the study, it remains to be seen whether our OMAM can work equally well or can identify the pathological effect of obesity in an obese population. Third, using different allometric equations to correct different Doppler parameters for a given individual is time-consuming. We have developed a software program that can be installed on echocardiographic workstations or individual cellphones to greatly facilitate the process of comparison between individuals and the differentiation between normal and abnormal corrected Doppler measurements. Finally, whether our OMAM equations are better at differentiating normal from abnormal hemodynamics in patients with heart failure requires further investigation.
《5. Conclusions》
5. Conclusions
In a large sample of healthy Chinese adults, we confirmed that different LV Doppler parameters allometrically correlated with one or more biometric variables, including age, height, weight, and heart rate, with different scaling constants and exponents. A novel OMAM was developed and a series of corrected normal reference values that were independent of biometric variables was established for 23 LV Doppler measurements. However, whether the OMAM equations can be applied to other ethnicities, obese subjects, or pathological conditions requires further investigation.
《Acknowledgments》
Acknowledgments
This work was supported by the Program of Introducing Talents of Discipline to Universities (BP 0719033), the State Key Program of the National Natural Science Foundation of China (82030051), the International Collaboration and Exchange Program of China (81920108003), the National Natural Science Foundation of China (81671703, 81770442, and 11771408), the Qingdao Key Health Discipline Development Fund (3311000000073), the People’s Livelihood Science and Technology Project of Qingdao (18-6-1- 62-nsh), and the Fundamental Research Funds for the Central Universities (201964006).
《Compliance with ethics guidelines》
Compliance with ethics guidelines
Guihua Yao, Xiangyun Chen, Wenjing Yang, Qing Zhang, Jing Liu, Huan Liang, Hui Sun, Yao Xu, Li Wang, Jinfeng Xu, Cheng Zhang, Fengrong Sun, Mei Zhang, Xueying Zeng, and Yun Zhang declare that they have no conflict of interest or financial conflicts to disclose.
《Appendix A. Supplementary data》
Appendix A. Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.eng.2021.05.007.











 京公网安备 11010502051620号
京公网安备 11010502051620号




