
《1.Introduction》
1.Introduction
Cartilage defects in orthopedic sites and in head and neck regions are frequently caused by trauma, cancer removal, aging, or congenital diseases. Since cartilage is avascular, aneural, and alymphatic, and contains only a sparse population of a single cell type (chondrocyte), its ability to regenerate after injury is hindered [1,2]. Major traditional procedures for cartilage repair include microfracture (marrow stimulation) [3], autografts [4], and autologous chondrocyte implantation (ACI) [5]. Although successful in some aspects, each of these methods has limitations such as unmatched property of the repaired region, lack of integration, and donor-site morbidity [6–8].
Tissue engineering provides a prospective alternative strategy by seeding chondrogenic cells into or onto biodegradable scaffolds in order to engineer cartilage for defect repair [9]. In orthopedic applications, the engineered cartilage is usually used to repair defects in an articular joint or in a meniscus in order to restore the joint’s load-bearing function and relieve pain. In head and neck applications, cartilage is usually engineered for the repair or reconstruction of an auricle, trachea, nose, larynx, or eyelid for an aesthetic or functional purpose. The challenges faced by the engineered cartilage for each application are quite different. In orthopedic applications, the engineered cartilage needs to integrate with the adjacent native cartilage as well as, in many cases, with the subchondral bone. The mechanical properties of the engineered cartilage should always match those of the adjacent tissue in order to enable survival and function within the biomechanically arduous joint environment [8]. The engineered cartilage also needs to cope with inflammatory mediators in cases with degenerative wounds. In head and neck applications, however, the engineered cartilaginous grafts are often required to be chondrogenically stable with superb biocompatibility so that they can survive and function in subcutaneous or intramuscular implantation sites, which lack chondroinductive cues and are characterized by acute immune response. In many cases, the engineered cartilage also needs to possess a specific shape with large volume and/or specialized function. As a result, engineering strategies to generate cartilage are usually quite different for each application. The statuses of preclinical animal investigations and of the clinical translation of engineered cartilage are also at different levels for each application.
Our group has been devoted to cartilage tissue engineering research for both applications for more than 20 years. Our specialty and research emphasis involve the in vitro regeneration of cartilage using different seed cell sources for the repair of different types of cartilage, and their preclinical large-animal evaluations. In this review, we provide an opinion piece on the developments in seed cell strategy, scaffold design, and preclinical animal investigation, as well as on the status of clinical translation, for both applications. We also summarize encountered challenges and future requirements.
《2.Tissue-engineered cartilage for orthopedic reconstruction》
2.Tissue-engineered cartilage for orthopedic reconstruction
Owing to upward trends in both life expectancy and youth obesity, a steady increase in the prevalence of osteoarthritis (OA) is expected [10,11]. Meanwhile, the incidence of athletic injury is also increasing. As a result, a major application of engineered cartilage is that of orthopedic practice to repair cartilage defects caused by traumatic or pathological injuries. Since the most important function of orthopedic cartilage is to bear weight, engineered neocartilage should ideally be able to: ① integrate not only with the subchondral bone, but also with the adjacent cartilage for stable load distribution and mechanotransduction; ② match the mechanical properties of the adjacent native cartilage in order to avoid tissue degradation caused by strain disparity; ③ be resistant to load under large deformations and motions; and ④ recapitulate the distinct zonal architecture in order to recreate the structure-function relationship of the native cartilage. The challenges of engineering biomechanically suitable cartilage have been thoroughly described in a review paper [8]. Moreover, engineered cartilage should be able to deal with the inflammatory environment of a degenerative cartilage.
Study activities to address these criteria have been sustained during the past two decades. The optimal cell source and scaffold are being explored. Preclinical large-animal investigations have been conducted. Many engineered cartilages for orthopedic reconstruction have realized clinical translation or even gained market access. However, despite the continuous progress in this field, no research activity has generated cartilage that can entirely mimic the properties and structure of native cartilage.
《2.1. Seed cell options for tissue-engineered cartilage for orthopedic reconstruction》
2.1. Seed cell options for tissue-engineered cartilage for orthopedic reconstruction
The implantation site of the engineered cartilage for orthopedic application is usually within the intra-articular space, in which chondroinductive cues in terms of cytokines and mechanical stimulations exist to promote the spontaneous chondrogenesis of the implanted cells and maintain their chondrogenic phenotype and function. Therefore, several different seed cell options exist: Chondrocytes [12], mesenchymal stem cells (MSCs) from different sources [13,14], (induced) pluripotent stem cells [15], and even fibroblasts [16] were reported as seed cell candidates to engineer cartilage for orthopedic applications. However, no consensus has been reached on which is to be accepted as the optimal cell source for current orthopedic cartilage engineering. Our group mainly focuses on two of the most clinically applicable seed cell sources: chondrocytes and MSCs.
2.1.1. Chondrocytes
Chondrocytes, the resident cartilage cells that are essential for cartilage-specific extracellular matrix (ECM) production, represent a logical choice of seed cells for cartilage engineering. Isolating chondrocytes from the joint surface is difficult, and would cause secondary injury leading to OA. Therefore, researchers have considered using non-articular “heterotopic” chondrocytes such as nasoseptal chondrocytes or auricular chondrocytes as an alternative cell source, since they are easier to harvest, associated with lower donor-site morbidity, and possess a higher proliferation rate [17–20]. However, it remains unclear whether heterotopic chondrocytes would produce cartilage with a desired type (such as hyaline cartilage) and function during defect healing. Chondrocytes from OA cartilage have also been tested as a seed cell candidate [21–23]. To use chondrocytes as a seed cell source, researchers need to deal with the issue of dedifferentiation by means of, for example, 3D microcarrier suspension culture [24,25], chondrocyte sorting [26], cytokine stimulation [27], or reduced oxygen tension [28], although too-extensively expanded chondrocytes may lose their capacity to re-differentiate [29]. Moreover, as evidenced in our previous study, chondrocytes may fail to form bone tissue in the subchondral bone region of an osteochondral defect (Fig. 1) [12,30].
2.1.2.Mesenchymal stem cells
To overcome the limitations of chondrocytes, MSCs gradually became the focus of many researchers [31]. MSCs can be harvested from a number of sources that do not affect cartilage activity, maintain multipotency after numerous expansions, and can be differentiated to generate both cartilage and bone—making the tissue-specific repair of osteochondral defects possible (Fig. 1) [30,32]. The immunosuppressive properties of MSCs, which are still maintained after their chondrogenic commitment, make off-the-shelf allogenic application practical [33,34]. Nevertheless, using MSCs as an alternative cell source for articular cartilage repair also presents several limitations, such as: low cell numbers of MSCs in the bone marrow or other donor tissue; the necessity for their careful characterization; the presence of several cell subpopulations; the content of already committed cells; the time-consuming chondrogenic differentiation procedure; the instability of the chondrogenic phenotype; and the uncontrolled differentiation in other lineages, particularly in view of the influence of inflammatory mediators in injured cartilage [18]. Moreover, neocartilage engineered from MSCs is reported to be epigenetically less similar to autologous cartilage than the engineered cartilage produced from primary chondrocytes [35]. Due to these limitations, safe regulations for using MSCs in a wide clinical application are difficult to make.
《Fig. 1》
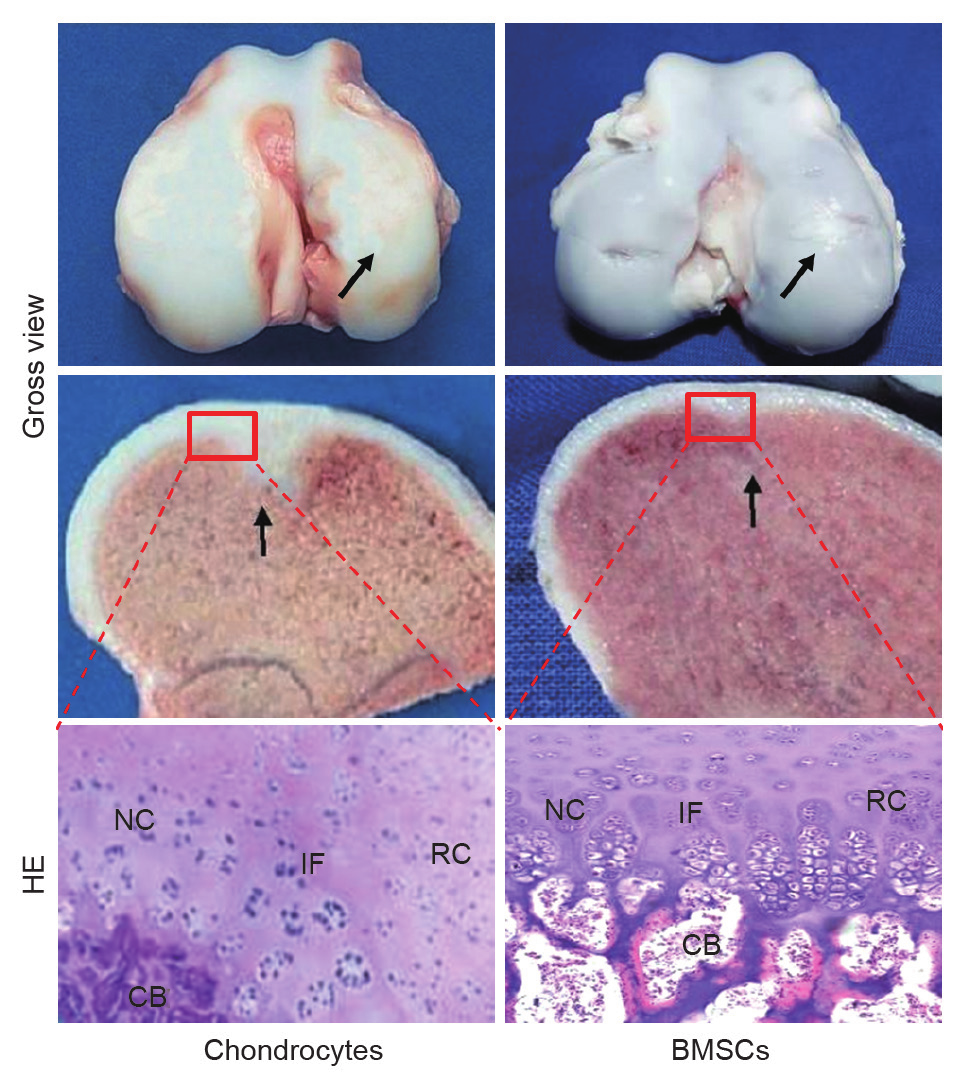
Fig. 1. Repair of autologous pig osteochondral defects by polyglycolic acid (PGA) scaffold loaded with chondrocytes or bone marrow stromal cells (BMSCs), respectively. Both cells realized cartilage repair with a smooth surface. Chondrocytes failed to realize tissue-specific repair in the subchondral region. HE: haemotoxylin and eosin; NC: native cartilage; IF: interface; RC: regenerated cartilage; CB: subchondral bone. Some of this data was published in Refs. [12,30].
《2.2. Scaffold options for tissue-engineered cartilage for orthopedic reconstruction》
2.2. Scaffold options for tissue-engineered cartilage for orthopedic reconstruction
2.2.1. Hydrogel scaffold
In orthopedic applications, hydrogels were first applied for the minimally invasive repair of focal cartilage lesions through injection or arthroscopy. As a scaffolding material for cartilage engineering, hydrogels have many advantages: They can exhibit similar mechanical, swelling, and lubricating behavior to articular cartilage [6]; their viscoelastic nature facilitates the transfer of mechanical loading [6]; and they allow their loaded cells to take on a spherical morphology, which is characteristic of the chondrogenic phenotype [36,37]. Cell-laden hydrogels have also been extensively investigated for use as bioink for the 3D bioprinting of cartilage with biomimetic structure and function [38,39]. Over the past decade, advanced hydrogels have been designed that are photosensitive [40–42], thermoresponsive [43,44], or self-assembling [45,46], or that permit the controlled release of chondroinductive factors [47] or chondroprotective drugs [48,49]. The combined application of hydrogels with other types of scaffold has been encouraged [50]. However, current designs of novel hydrogels mainly focus on certain aspects of the material property, and thus fail to replicate the complexities of the entire chondrogenic niche. Therefore, enhanced collaboration of material scientists with experts from other related fields in tissue engineering is of vital importance to enable the development of hydrogels with balanced mechanical properties, electrical conductivity, degradation rate, biocompatibility, and chondroinductive properties. Merging novel hydrogels with advanced technologies such as 3D bioprinting is also a promising trend [51].
2.2.2. Solid scaffold
Regarding the liquid or gel form of a hydrogel scaffold, many researchers (including our group) prefer to use solid scaffolds to engineer cartilage for large, uncontained defect repair. Solid scaffolds can also be categorized into natural and synthetic derivatives. Natural scaffolds such as collagen sponge, decellularized cartilage, and small intestinal submucosa (SIS) have the benefits of biofunction and signaling cues. Among these, collagen sponge is currently the scaffold that is most widely used to repair cartilage in clinical applications. Synthetic materials are easily processed, with superb batch consistency, and their mechanical and chemical properties can be easily tailored. Since the articular capsule can block some of the immune response cells, some synthetic materials that may induce a serious host response in the subcutaneous site can be used as a tissue engineering scaffold for orthopedic application [52]. One example is polyglycolic acid (PGA), which has been shown to be a superb carrier for many types of cells, and which has been extensively used by our group to engineer cartilage in vitro and in vivo, using different types of seed cells for articular cartilage lesion repair or meniscus reconstruction [12,16,30]. To harness the merits of different scaffolds, the combined application of naturally derived material with a synthetic scaffold became a reasonable approach. Applications of multi-phasic scaffolds are emerging, especially in attempts toward osteochondral repair [53–55]. However, before clinical application, the efficacy of these biomaterials must be proven through long-term preclinical large-animal investigations.
《2.3. Preclinical large-animal studies of tissue-engineered cartilage for orthopedic reconstruction》
2.3. Preclinical large-animal studies of tissue-engineered cartilage for orthopedic reconstruction
Preclinical immunocompetent animal investigation is an essential step to assess whether the engineered tissue can be used in clinical settings. During the past two decades, we have successfully repaired cartilage or osteochondral defects in pigs [12,30]. We have also repaired meniscus defects in dogs (Fig. 2, unpublished data). For orthopedic applications, we chose an animal model mainly based on its joint anatomy and cartilage volume (area and thickness). As recommended by Ahern et al. [56], other criteria such as handle difficulty, husbandry requirements, cost, size, and skeletal maturity time should also be considered.
《Fig. 2》
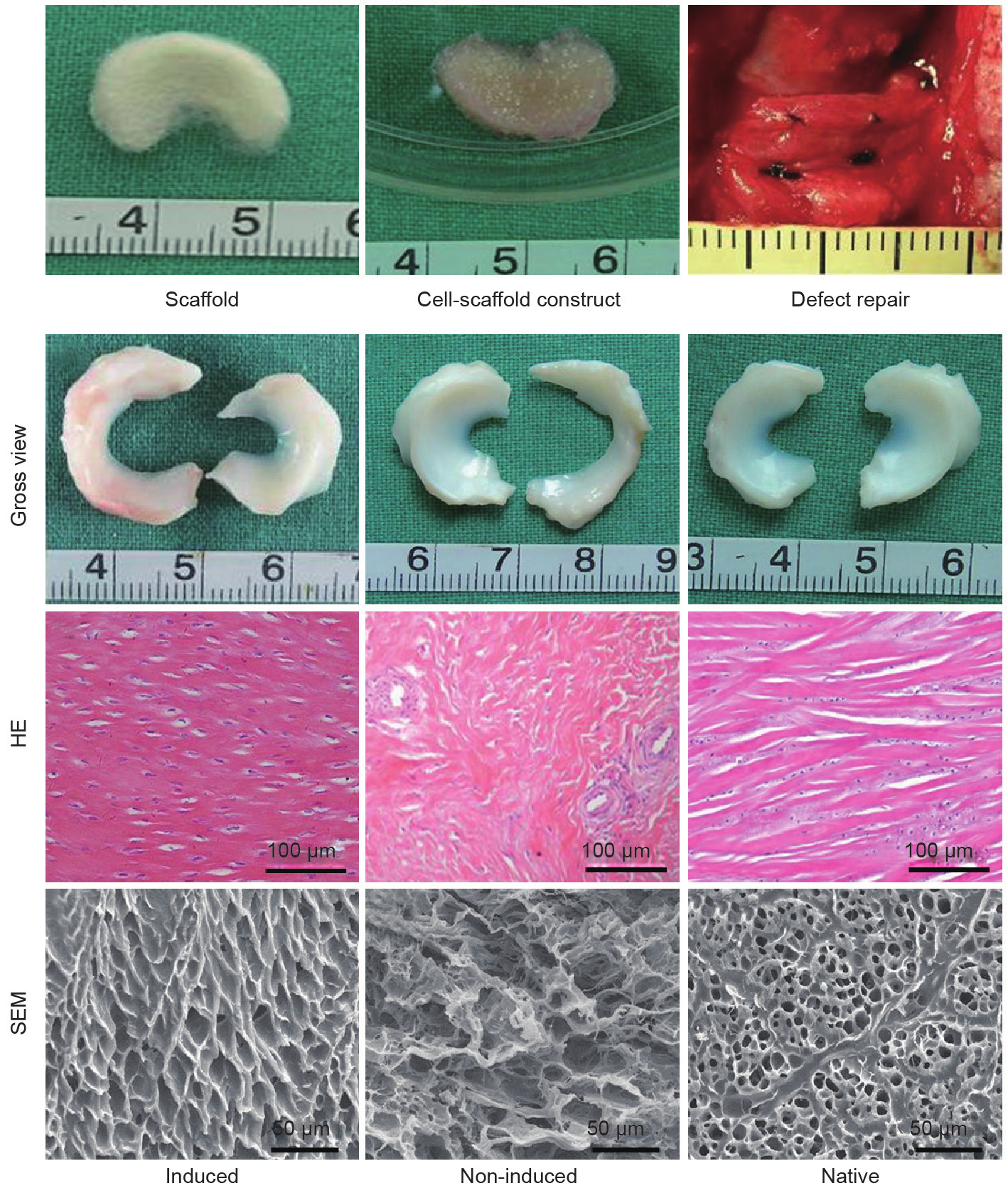
Fig. 2. Repair of autologous dog meniscus defects by a PGA scaffold loaded with chondrogenically induced fibroblasts. Fibroblasts were chondrogenically induced with cartilage-derived morphogenetic protein-1 (CDMP1) and seeded into a meniscus-shaped PGA scaffold, with non-induced cells as the control. At 3 months post implantation, the meniscus generated by samples from the induced group resembled a native meniscus in terms of gross appearance, histological staining, and microstructure, which was revealed by scanning electron microscope (SEM) observation.
Aside from the quality of the engineered cartilage, many other factors can greatly influence the outcome of large-animal studies. For example, in our recent attempt to repair osteochondral defects in a porcine model, we failed to obtain reasonable results because we had destroyed the physical loading condition by creating too many defects in one animal. Effective fixation of the engineered cartilage into the defect is also critical, and this should be done without introducing additional factors that affect the study design.
In fact, because too many factors could influence the results of a preclinical animal investigation, comparison among different studies became very difficult. Therefore, standardization of study design and outcome parameters such as histological, biochemical, and biomechanical evaluations should be established [56]. Moreover, although large-animal investigations provide valuable data for predicting the efficacy of a novel treatment strategy, one should always bear in mind that no animal model permits direct application to humans [52]. For example, most defects created in a largeanimal model are fresh wounds; however, in clinical settings, we need to deal with chronic defects with a disturbed local environment that is quite different from the environment in newly created fresh wounds [57].
《2.4. Clinical application of tissue-engineered cartilage for orthopedic reconstruction》
2.4. Clinical application of tissue-engineered cartilage for orthopedic reconstruction
Tissue engineering principles are currently being applied to clinical application mostly in the form of ACI or using similar techniques [58]. Related products such as Carticel® and Hyalograft® C have already gained access to the market for the treatment of traumatic cartilage lesions. Current, clinically available tissue-engineered cartilage products have been thoroughly described in a recent review paper [59]. However, despite refinements in technique, ACI-type technologies have failed to demonstrate significant clinical benefit over older techniques such as microfracture, except perhaps for larger lesions [58]. Moreover, these technologies cannot treat large defects or those associated with advanced diseases such as OA [60], and show no potential for the reconstruction of an entire structural unit such as a joint head or meniscus. As a result, researchers are investigating more advanced technologies with the ultimate goal of safe, standardized, cost-effective and good manufacturing practice (GMP)-compliant production of large-scale cartilage grafts [60]. Nevertheless, due to difficulties in evaluating the quality of the engineered cartilage, including its safety, cost-effectiveness, and complications in a procedure, most of the new developments in cartilage tissue engineering have yet to translate into measurable clinical gains [58].
《3.Tissue-engineered cartilage for head and neck reconstruction》
3.Tissue-engineered cartilage for head and neck reconstruction
In addition to orthopedic applications, engineered cartilage can be used in head and neck reconstruction to treat cartilage defects in the auricle, nose, eyelid, trachea, and so forth. Our group mainly focuses on auricular reconstruction and long segmental trachea reconstruction, which are among the most representative and difficult cases in head and neck application and which may provide valuable reference for other applications. Unlike the engineered cartilage for orthopedic applications, the engineered cartilages for head and neck reconstruction are usually required to possess complex forms; their implantation sites are non-chondrogenic and characterized by aggressive immunological responses, making the choice of seed cells and scaffolds quite limited. For the same reason, preclinical evaluations and proof-of-concept clinical studies of engineered auricles or tracheas are limited, and vast clinical applications are not yet in sight.
《3.1. Seed cell options for tissue-engineered cartilage for head and neck reconstruction》
3.1. Seed cell options for tissue-engineered cartilage for head and neck reconstruction
Chondrocytes are the most popular choice for seed cells to engineer cartilage for head and neck reconstruction. One reason for their popularity is that proliferative chondrocytes can be easily isolated from the auricle or nasal septum without causing functional damage to the donor tissue, as compared with the isolation of articular chondrocytes from the knee joint [61]. Another important reason is that cartilage engineered from stem cells is unstable and predisposed to ossification in the subcutaneous or intramuscular implantation site of the head and neck regions [62,63]. In this case, co-culture of chondrocytes with MSCs may prove to be a more reasonable seed cell strategy.
3.1.1. Chondrocytes
Chondrocytes are usually isolated from the nasal septum (hyaline cartilage) or auricle (elastic cartilage) to engineer cartilage for head and neck reconstruction. In particular, for auricular reconstruction for patients with microtia, the deformed ear cartilage, which would otherwise be discarded, provides an ideal seed cell source without harming healthy cartilage [64,65]. Chondrocytes are traditionally considered to have low proliferation ability. However, researchers have found that chondrocytes isolated from the nasal septum or auricle were more proliferative than previously expected [66,67]. More importantly, engineered cartilage formed by these chondrocytes maintains stable phenotype and function without shrinkage or ossification in a subcutaneous environment. Although they are proliferative, however, these cells still have dedifferentiation issues. We found that chondrocytes from microtia cartilage stop expressing collagen II and aggrecan at passage 1 in monolayer culture and at passage 2 in pellet culture [66]. As a result, in order to achieve a sufficient quantity of functional chondrocytes, procedures to re-differentiate the dedifferentiated cells are necessary. However, these procedures may involve the application of multiple chemical or cytokine factors, which may introduce safety concerns for future clinical application.
3.1.2.Mesenchymal stem cells
Owing to the non-chondrogenic implantation site in head and neck applications, in which stem cells are predisposed to terminal ossification, only a limited number of reports have described successful regeneration of stable cartilage using individual MSCs in a subcutaneous site [62,68]. Co-culture of MSCs with a small portion of chondrocytes proves an effective seed cell strategy to form stable cartilage in a non-chondrogenic environment [69–71]. Our group has successfully generated human ear-shaped cartilage in a nude mouse model using bone-marrow-derived MSCs co-cultured with microtia chondrocytes [66]. Co-culture can reduce the demand for chondrocytes, minimizing the donor-site morbidity left by chondrocyte harvesting. It is also hypothesized that MSCs may be able to adjust the local immune environment, reducing the risk of the engineered cartilage being attacked by the subcutaneous host response. The mechanism under which co-culture promotes stable chondrogenesis has many directions. Our group has demonstrated the direct chondrogenesis of green fluorescent protein (GFP)-labeled MSCs during co-culture with chondrocytes, and has illustrated that soluble factors produced by chondrocytes are the key reason for chondrogenesis of the MSCs [70]. On the other hand, a trophic effect of MSCs has also been demonstrated to promote proliferation and ECM production of chondrocytes [72,73]. Direct cell-cell contact and communication through gap junctions may also play a role in MSC’s chondrogenesis [74]. However, the question of which is the dominant mechanism is yet to be determined.
《3.2. Scaffold options for tissue-engineered cartilage for head and neck reconstruction》
3.2. Scaffold options for tissue-engineered cartilage for head and neck reconstruction
The subcutaneous or intramuscular implantation site of head and neck applications is characterized by an acute host response. As a result, most successful regenerations of subcutaneous cartilage are based on scaffold-free chondrocyte suspension [75,76]; an engineered cartilage sheet [77,78]; or material with superb biocompatibility, such as collagen [79,80]. To provide chondrogenic cues for the stable chondrogenesis of stem cells in a subcutaneous environment, the application of decellularized chondrocyte ECM or cartilage is also a common option [81]. As a great many cases in head and neck reconstruction require the engineered cartilage to have specific forms, such as an auricle, trachea, or nose, synthetic scaffolds with strong mechanical properties that are easy to shape and that will not shrink during culture are preferred. Our group has been using PGA to engineer cartilage for auricular and trachea reconstruction for the past 20 years. To overcome the inflammatory reaction induced by PGA, we proposed in vitro pre-cultivation in order to allow sufficient degradation of the PGA scaffold before implantation [82,83]. Researchers have also managed to generate a compound scaffold with both strong mechanical properties and superb biocompatibility by using slowor non-degrading material as an inner core to support the shape, and then wrapping the inner core with biocompatible natural materials that act as a cell carrier for cartilage formation [80,84]. However, the introduction of slowor non-degrading materials as an inner core complicated the case by making it difficult to determine whether the generated chimeric graft was an engineered tissue with bioactivity, or just a device or prosthesis supporting the shape. It may also be necessary for a non-degrading inner core to deal with the possibility of extrusion. Therefore, a scaffold with good mechanical properties, easy shaping control, and superb biocompatibility is urgently needed. Such a scaffold might be manufactured by modifying the current characteristics of a scaffold—for example, by the controlled release of immunomodulating drugs [48,85]. In light of future alternatives, state-of-the-art current 3D bioprinting procedures may offer one-step generation of cartilage with structural integrity [86].
《3.3. Immunocompetent animal studies of tissue-engineered cartilage for head and neck reconstruction》
3.3. Immunocompetent animal studies of tissue-engineered cartilage for head and neck reconstruction
Current reports on engineered cartilage for head and neck reconstruction are mostly in the stage of in vitro or nude mouse investigation. Only a limited number of reports have described successful attempts to engineer an auricle or trachea in immunocompetent animals [80,82,87]. One major reason for this lack of success is that the acute immune response in the subcutaneous or intramuscular implantation site will attack an implanted graft that has been engineered using a scaffold with suboptimal biocompatibility [83,88]. For head and neck reconstruction, the engineered cartilage needs to have a large size with a specific form (such as an auricle) or function, which further complicates the case. The engineering of a human ear-shaped cartilage is one example. As early as 1997, the successful generation of a human ear-shaped cartilage in a nude mouse was reported [89]. However, it was only recently that the successful generation of a full-sized human ear-shaped cartilage was reported, this time in an ovine model [80]. Structural recapitulation is only one step toward success. Many cases have rigid functional demands. Trachea reconstruction provides an example: Our group reported the successful subcutaneous generation of tubular cartilage in an autologous rabbit in 2009 [82]. However, when using this tubular cartilage to repair a segmental tracheal defect in an autologous rabbit, we encountered problems of airway stenosis (caused by the overgrowth of granulation tissue), airway collapse (caused by cartilage softening), and mucous impaction (mainly caused by a lack of epithelium). For the functional repair of a tracheal defect, we applied silicone stents to depress granulation overgrowth and prevent airway stenosis, and then used intramuscular implantation and transplantation with a pedicled muscular flap to establish a stable blood supply in order to maintain the tubular cartilage structure and accelerate epithelialization. By combining these strategies, we finally realized the long-term functional reconstruction of segmental tracheal defects in a rabbit (Fig. 3) [87]. However, reproduction of this result in a preclinical goat model has not yet been achieved because a goat has a more acute immune system, and the post-operative care is more demanding [83]. Clearly, the challenges for preclinical animal studies of engineered cartilage for head and neck reconstruction are profound. Engineering technology needs to be improved to provide cartilage with a large volume, strong mechanical properties, and superb biocompatibility. Intimate collaboration with surgeons is also critical, as the anatomical structures in the head and neck regions are complicated.
《Fig. 3》
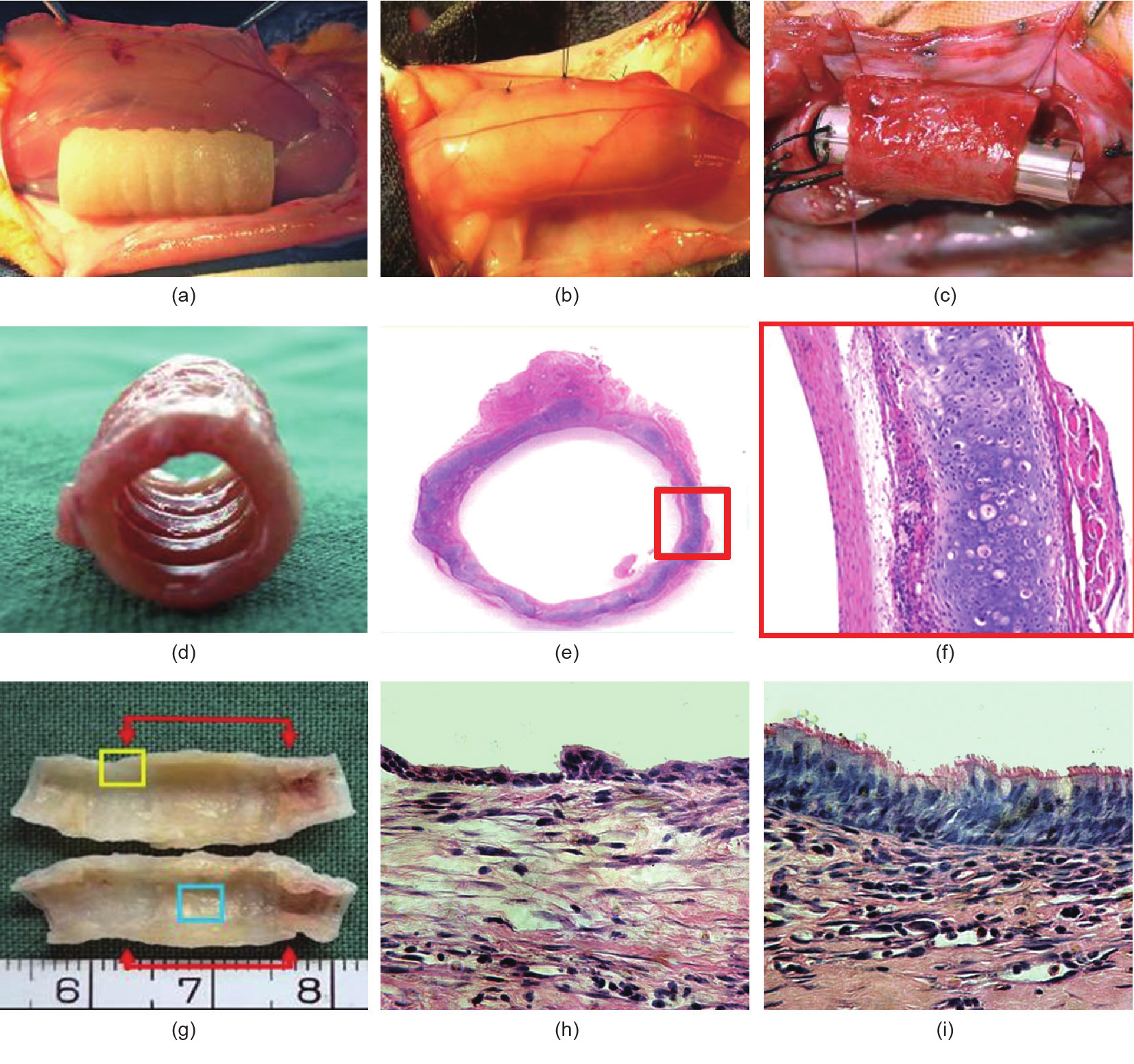
Fig. 3. Functional reconstruction of a segmental tracheal defect by pedicled tissue-engineered trachea in a rabbit model. (a) Tissue-engineered trachea; (b) the tissueengineered trachea wrapped by the sternohyoid muscle for vascularization; (c) the muscle-pedicled trachea used to repair a segmental defect of the trachea with a silicon tube as a stent; (d) the tissue-engineered trachea after 4 weeks of reconstruction; (e) HE staining of (d); (f) high magnification of the red frame of (e); (g) cross-section of the tissue-engineered trachea after 6 months post-reconstruction, showing a fine interface healing with the native trachea (yellow frame: interface, blue frame: engineered trachea); (h) HE staining showing epithelium ingrowth at 2 weeks post-reconstruction; (i) HE staining showing epithelium ingrowth at 8 weeks post-reconstruction. Some of the data has been published [87].
《3.4. Clinical application of tissue-engineered cartilage for head and neck reconstruction》
3.4. Clinical application of tissue-engineered cartilage for head and neck reconstruction
Notable recent clinical events regarding engineered cartilage in head and neck regions include:
• Tissue-engineered trachea: In 2008, Macchiarini et al. [90] reported the first clinical application of a tissue-engineered, stem-cell-based, decellularized trachea to treat a 30-year-old woman; the 5-year follow-up results were reported in 2014 [91]. In alternative efforts to avoid the need for a donor trachea, investigators have also utilized a nanocomposite material as the scaffold for an engineered stem-cell-based trachea for patient use [92,93]. However, the efficacy and authenticity of these methods turned out to be quite controversial.
• Tissue engineering in auricular reconstruction: In 2009, Yanaga et al. [75] described a two-stage ACI-type approach that injected massively expanded microtia chondrocytes into the lower abdomen of patients to form cartilage blocks, which were then hand-carved into ear frameworks for auricular reconstruction. No report described the direct engineering of human ear-shaped cartilage based on cells and pre-shaped biodegradable scaffolds for clinical application.
• Tissue engineering in nasal alar lobe defects: In 2014, Fulco et al. [94] reported a first-in-human trial in which nasal septum chondrocytes were seeded onto fibrous collagen scaffolds in order to engineer cartilage pieces for the repair of nasal alar lobe defects in five patients. No report has described total nasal reconstruction based on tissue engineering methodologies.
The efforts listed here are only proof-of-concept clinical translations; vast clinical application still has a long way to go.
《4.Conclusions》
4.Conclusions
After more than 20 years of continuous development, cartilage engineering has achieved some notable progress. Many basic bioengineering investigations have made breakthroughs, and the number of ongoing clinical studies is increasing, bringing the prospect of tissue regeneration closer to reality. Nevertheless, the process of translating proof-of-concept research into preclinical or clinical investigation gives rise to escalated challenges. For orthopedic applications, in which tissue engineering may be closer to widespread clinical adoption, facilitated integration of the engineered cartilage with both subchondral bone and the adjacent cartilage should be ensured. The mechanical properties of the engineered cartilage should also match those of the adjacent tissue in order to provide an immediate and long-term load-bearing function. The harsh degenerative environment of OA or a chronic wound should also be taken into consideration. For head and neck applications, proof-of-concept clinical translation is thriving, but vast clinical application is not yet in sight. The engineered cartilage should be extremely biocompatible in order to avoid the acute immune response of the subcutaneous or intramuscular implantation sites. Moreover, the engineered cartilage should accurately recapitulate both the structural and the functional properties of the tissue being reconstructed. For both applications, it is now more critical than ever to demand intimate collaborations of experts from developmental biology, cell biology, and material science, along with surgeons and regulation makers, so that the scope of scientific understanding can be effectively expanded into actual application.
《Compliance with ethics guidelines》
Compliance with ethics guidelines
Yu Liu, Guangdong Zhou, and Yilin Cao declare that they have no conflict of interest or financial conflicts to disclose.











 京公网安备 11010502051620号
京公网安备 11010502051620号




